 Abstract
Abstract
Advances in online technology have offered us an immense possibility to save precious therapeutic time and a better insight into the pathology of our clients. By asking them to submit their personal history through a facile, user friendly online form from the safety and comfort of their home, we will have an acceptable and decent profile long before they walk in our office. Another benefit of this procedure is that we are provided with a general overview of data that could make sense in our practice and contribute to make it even better and more effective.
Introduction
If you look at the mean average of individual sessions in regression therapy, you will see that people come to us up to three times at best which is a very low rate. This makes our first session and our intake interview the most crucial encounter with our clients. If that session is successful, we lay the ground to build a potentially healthy therapeutic cooperation. For me it was always important to get a thorough interview from my clients. But I had difficulty listening carefully on the one hand, and writing down my notes on the paper questionnaire I was filling in. The art of recording in paper as well as in mind is a challenging feat which requires profound skills from the therapist, an acute alertness and fast processing of incoming information. The risk of missing crucial hints is imminent and that may affect our session negatively.
By employing the online intake form (OIF) beforehand we have the luxury of studying the personal history of our client and we have the ability to highlight the “gray” areas that need further illumination and analysis when we finally meet in person. Meanwhile, we have the convenience to focus on the body language, gestures, and physical signs that may reveal a lot more about the pathology of our clients.
The advantage of the OIF is that it is not written on stone. In other words, we can always review, revise and update our questionnaire and in that way keep up with societal trends and developments. Another advantage is that if the OIF after review, revision and editing by colleagues can take a standardized format, then it would allow for statistical analyses and processing of information in the future.
The inspiration to shift from paper to online was triggered by our colleague Prakriti Saxena Poddar. During a workshop in the 6th World Congress of Regression Therapy she presented the usage of the online forms. This free online service provided by Google Forms is a very facile and easy to build procedure. As soon as I returned to Greece, I started employing it in my practice. Since that time I have had 350 inputs. Since, CoVid-19 has locked us down and placed a halt in the life as we used to live it, I took the opportunity to share all this information with our colleagues in the hope of a more extended use and acceptance of OIF in the future.
Discussion
I have set up my OIF in 15 sections, which contain 220 fields. You can all have online access to this if you follow this link: https://tinyurl.com/y49hu32f Many of the questions have been adopted by many books I have read, but the most important are listed on the reference section.
The first section concerns our client’s consent to store and process their personal data. If they do not consent to this, the OIF is not filled in, the process is aborted and thus we turn back to our traditional one to one approach. All colleagues (at least Europeans) who are interested in employing the service of OIF’s in their practice should first thoroughly study the GDPR (General Data Protection Regulation) guidelines for collecting and maintaining personal data.
The second section consists of the client’s contact information. Here we gather all the material in order to communicate with them. The risk of misreading notes or mishearing numbers diminishes. Here you also have the ability to automatically collect the emails of your clients and import them to your Mailchimp or any other similar email marketing platform for your Bulletin/Newsletter.
The third section concerns the way your clients found you. How did they resort to you? This could give you hints for further marketing strategies for attracting future clients.
The fourth section initiates the actual intake of personal data. In this section I have placed the independent variables like gender, age, level of education, etc., so they can be used in a possible statistical analysis in the future.
In the fifth section we start to get deeper into personal issues recording family history and childhood experiences. In the sixth section we enter in the aspects of leisure time. We want to see how our clients allocate their free time. What are their tastes concerning athletics, arts and culture?
We then move to the other aspect of life that takes one third of our lifetime, sleep. How are our clients experiencing their sleep, what is their relationship to their dreams? What is their connection to their unconscious?
Then we move to the eighth and ninth sections, the medical history of our client and their family. It is important to know these parameters before you place someone in trance. For instance, you should be very cautious if your client reports that they have had epileptic seizures in the past. Or you should reconsider accepting a client who has been hospitalized for schizophrenia.
The tenth section is only for women. Fertility issues, sexual problems, pregnancies and abortions are very important to know about before you begin a session. The eleventh section becomes more specific in recording modes of behavior even though some of the questions are also in former sections. Here you will find more questions of the IAPAS type (Initial Assessment of Possible Attachment Scale, (Komianos, 2011)) that concern the possibility of the existence of spiritual attachments within our clients.
The 12th section concerns an opportunity to record and file the so-called paranormal and metaphysical experiences that our clients usually do not disclose because of the fear of public contempt and ridicule. In my opinion mainstream psychiatrists should be held responsible for stigmatizing such universal and omnipresent experiences as pathological manifestations and signs of disorders.
The 13th section is devoted to recording the presenting issues of our clients. Here they clarify the reason of their visit to our office. The next section “Fill in the sentence,” consists of open-ended phrases, starting with a verb or a noun, so that our clients can fill in whatever feeling first comes into mind. Reading through the inputs I have found amazingly surprising sentences that reveal quite a bit about my clients.
The last section concerns the “Client Bill of Rights”. A clear-cut document of who you are, what you do, what services you provide and the codes of conduct that rule your practice. This has to be customized separately for each therapist. We all have different backgrounds, education, training, occupational history and experience. In this section, we have to be very transparent, coherent and sincere so that our clients know with whom they will be working and under what conditions. Present here the cost of the session, what the client’s privileges and rights are and how they should manage their expectations. All this should be clearly stated in this section.
Filling in such a form may take up to two hours. It may be more difficult for senior citizens or for people with low internet literacy, but it is the way of the future and by adopting to it, you save a significant amount of time. Another advantage of the OIF is that the clients (if they keep the link given to them by Google Forms at the end of the submission) can always return to the form and edit the material if they did not recollect something at the time they filled in the data.
A further important feature is that we, the readers and managers of the material, cannot alter or edit the inputs of our clients in anyway. This means that the material is preserved as it was input by our clients.
An additional function provided by Google Forms is that these data is automatically filed in an EXCEL type file called SHEETS, so you have an overview of all the data in one file.
So far, this service provided by Google Forms does not give you the opportunity to control and juxtapose data. You cannot easily tabulate how many females have phobias, or what the age group of those clients who have tattoos, or what the sleep patterns are of homosexuals, for example. Possibly such a service will be provided sometime in the future by specific companies that work with data. However, at this time Google Forms does offer us a good start.
Making Sense of the Numbers
First of all, the group represented in this paper is comprised of my clients who filled in the OIF from October 2017 to March 2020—30 months in total. The total number of clients is (N=350). Approximately 20 people who visited me in this particular period did not fill in the form—either because they did not have internet literacy, access to a valid internet account, or lacked trust placing information online. These people are not included in this study group.
Not all people filled in all of the answers in my OIF unless the questions were mandatory (i.e. age, sex, email, etc.). Our total sample consisted of 350 (N=350) participants, but not all of the 220 questions were answered. In cases that the number of people who reply is less than 320, I will specify the sample number within brackets, i.e. (N=123).
Almost one in two of my clients have come to me by way of word of mouth. The second most important route is the internet search (40%) while the third one is TV shows and interviews (14%). My book has only brought 6% of my clients, while radio interviews constitutes less than 1% of the sample. Lectures either in my community or in other places, have brought in less than 5% of my clientele. Do not be confused by the figures if when added up look as if they surpass 100%. Clients may first see you on a show, or hear your name, or read your book, and then look further on about you on the internet. Roots of communication are not exclusive.
Two thirds of my clients are female and one third are male. Eighty-seven percent are right-handed while 9.1% are left-handed and 3.1% are ambidextrous. The interesting figure is that almost 10% of the world population is left-handed so my figures are very close to the global average (Papadatou-Pastou, et al, 2020).
More than half of my clients are graduates of college and universities while 16.6% have a master’s degree and 2.3% have a PhD. So almost two thirds of my clients are highly educated persons.
Almost one in three are single, 20% are married, 25% are in a relationship, while 17% are divorced. 2% are widowed persons. 91% of my clients are heterosexual while 4.4% are homosexual and 2.9% are bisexual. These figures are certainly not consistent with those given by Dr. Alfred Kinsey in his Sexual Behavior in the Human Male (p. 651).
Sleep quality seems to be dispersed like a bell shape curve. Almost five percent of the participants have terrible sleep patterns while almost fifteen percent are very much satisfied by their sleep quality. The rest of my clients are somewhere in between these two extremes.
Almost 10% of our group have no ability to recollect any of their dreams while at the other end approximately 20% recall their dreams very often. About 60% of my clients see both pleasant and unpleasant dreams. Unfortunately, 5.7% see only nightmares and unpleasant dreams.
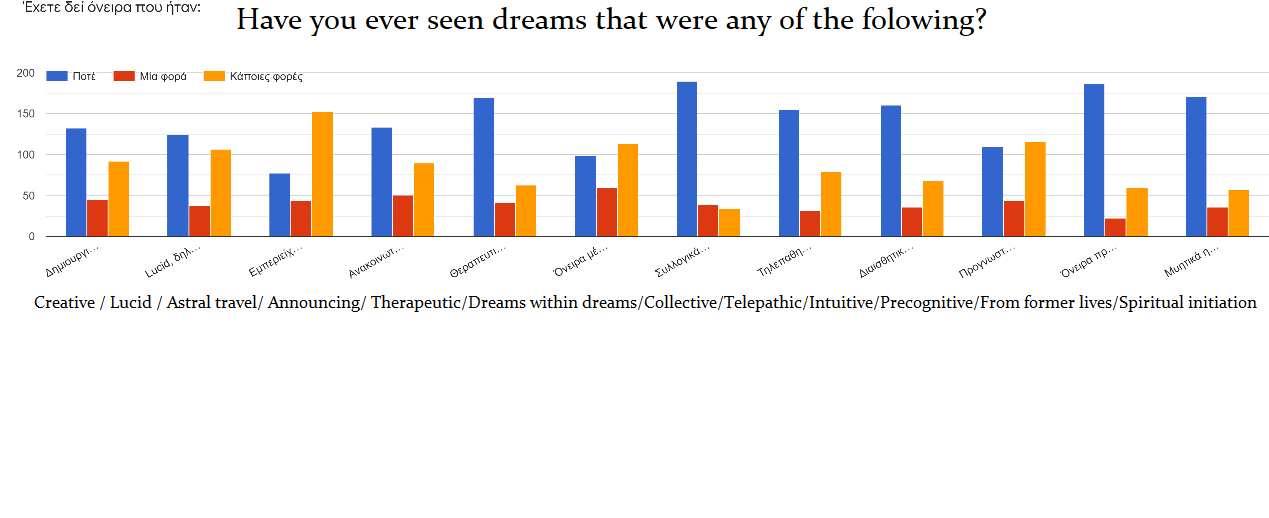
I also have a section about dreaming that is based on the classification of extraordinary dreams as listed by Dr. Stanley Krippner (Krippner et al. 2002). These dreams are split into twelve categories as listed below:
| Extraordinary dreams
|
Never | Once | Sometimes |
| Creative dreams that provide solutions to problems
|
131 | 45 | 90 |
| Lucid dreams whereas the subject takes control of the turn of the dream.
|
124 | 37 | 105 |
| Dreams where astral projection takes place
|
78 | 44 | 149 |
| Announcing dreams. Like announcing a coming pregnancy, death or another significant event.
|
133 | 51 | 87 |
| Therapeutic dreams that show us something about our state of health
|
168 | 39 | 63 |
| Dreams in dreams in which we have the wrong impression of waking up
|
98 | 58 | 112 |
| Collective dreams where at least two people report similar dream experiences | 187 | 38 | 34 |
| Telepathic dreams in which we identify with the thoughts of a person who is far away from us | 152 | 32 | 79 |
| Intuitive dreams in which we perceive events that took place at a long distance and that we would have no normal way of knowing | 159 | 36 | 66 |
| Predictive dreams that provide information about events that have not yet happened | 110 | 33 | 113 |
| Dreams of past lives and what seem to belong to circumstances from previous incarnations? | 184 | 21 | 59 |
| Dreams of spiritual initiation and teaching | 169 | 35 | 56 |
Thirty percent of the group have never seen a nightmare while 40% have seen repeated nightmares even though they are not identical. A very interesting figure is that 23% have at least sleepwalked once in their lifetime. While 17.6% still talk during their sleep. Both of these factors are strong indicators of high hypnotizability (Kappas, 2001).
Another interesting fact is that half of my clients, at least once in their life, have experienced sleep paralysis. Furthermore, some people who describe their experiences describe the feeling of a presence and/or an entity suppressing them at the area of the chest. In elaborating the particular figures, we come very close to the figures provided by anthropologist David Hufford (Hufford, 1982) who claimed that at least thirteen percent of the total population have undergone this encounter with the “Old Hag” at least once (Hufford, 1982, pp. 51-55).[1]
An indicator of chronic stress disorder is the clenching of the jaw during sleep. One third of my clients have never experienced this. However, all the rest have done so and about 18% of them clench their teeth very often.
Further on I have a question about spontaneous awakening. And even though I was under the impression that everyone had the ability to awaken without the help of an alarm clock I realized that at least 5% of my clients cannot. Almost one in five persons in the sample have been born by caesarian section. At least once in their life till very often persons had enuresis (peeing in bed) during their sleep. A quarter of the group “had a long-term illness, issue, or health condition that had not been adequately diagnosed.”
Most of the clients (N=281) in the group had first visited mainstream therapists. Half of them had visited psychotherapists, 22% psychoanalysts, 14% counselors, 10% neurologists, 12% other hypnotherapists and 35% alternative therapists. Most clients had visited more than one therapist. Only 15% of my sample had had a visit with another regression therapist.
One in two out of those clients who have a medical diagnosis (N=150) were diagnosed with depression. Thirty-five percent have been diagnosed with anxiety disorder and 9% with bipolar disorder. All other diagnoses have small percentages. One in three of the group have tried homeopathy. The effectiveness of it is dispersed dubiously, but more than half of the patients have a positive stance.
Another interesting number is one in three persons (N=144) had at least one memory gap in their lifetime. As far as sexual behavior is concerned it is no surprise that 29% of this sample are sexually inactive. Only 8.7% are very active. The rest are somewhere in between. Sixty-eight percent report that they are monogamous, 17% occasionally monogamous, 9.8% occasionally polygamous and 4.5% are polygamous. As far as satisfaction is concerned one in four have very little satisfaction from their love life while only 10% are very satisfied. The rest belong somewhere in the middle.
One in four persons of my sample are omnivorous, 7.6% are vegetarian, while 2.9% are vegan. Amazing to me is the fact that almost one in two consider themselves sensitive to the moon cycle.
In a far smaller part of our group (N=104), 36% have been diagnosed with dyslexia,
36.5% have attention deficit and 24% are hyperactive. More than half (62%) of the group are emotionally moved and/or even cry (30%) when they watch a movie demonstrating a high factor of suggestibility and hypnotizability.
Three quarters of the group are frequent daydreamers and the majority of them find it very difficult to tell a lie. On the other hand, 8.7% can very easily make up a lie. .
Fifty-eight percent are procrastinators and last-minute persons. Dogs (261/350), cats (188/350) and birds (144/350) win a place in the hearts of those sampled. As expected, serpents, rats and insects occupy a minor part of their heart.
As far as the women in the study are concerned (N=253) 16.6% have had at least one abortion while 9% have fertility problems. One in three women (N=237) always has an orgasm while engaged sexually, 38.4% have orgasms most of the time, while at the other end 3.4% have never experienced an orgasm.
Fifty-nine percent feel low vitality and lack of vigor, 27.4% feel higher vitality and vigor. Fifty-six percent do have mood swings for no apparent reason. Forty-eight percent have had depression sometime in their lives. Twenty-three percent have considered thoughts (no attempts <1%) of suicide. Sixty-one percent conclude a task once they undertake it. Thirty-four percent are prone to have minor accidents, make mistakes, stumble upon things often or do things fall off their hands, for no reason. Thirty-seven percent have at least once heard an internal voice telling them what to do. Thirty-six percent have sometimes felt that the thoughts they have in their mind are not really their own. Sixty-two percent have lost from life a loved one that they were emotionally attached to.
Forty-five percent have experienced an accident or a traumatic experience that shocked them.
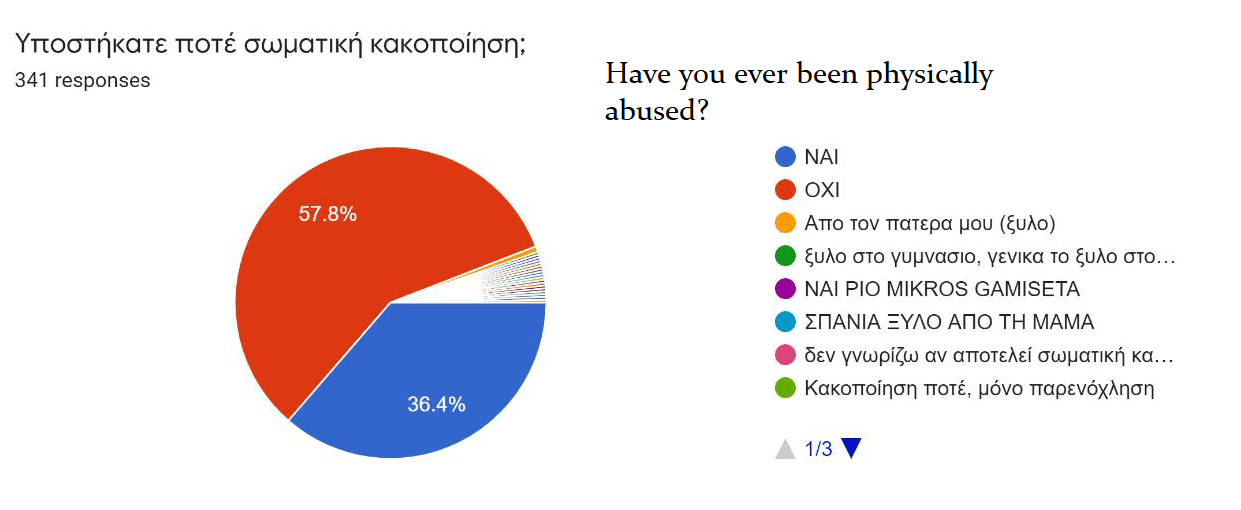
Thirty-six percent have experienced physical violence, while 13.4% have experienced sexual assault. Twenty-seven percent have a problem being touched on specific areas of their body. Forty percent (N=317) have had either compulsions or obsessive behaviors.
It seems that the majority of my clients in this study, 35.5%, perceive reality mostly kinesthetically, 31.2% are primarily visual, while 15.3% are auditory, while primarily olfactory are only 5.5%, about 10% say that they perceive all of the above.
At least 40% of the group have had the sense of being watched. Ninety-three percent gave me permission to touch them on a specific part of their body in the event I considered that there was a need for this during the session.
A surprise to me was that 38.8% of these clients have reported having a birthmark. However, upon inspection I surmised that this claim was not always the case, despite the fact that the true incidence of birthmarks is far higher than expected by the known statistics (Stevenson, 1997). Another surprise is that 11.9% reported a birth defect, but again, upon inspection, the actual percentage is lower.
Fifty three percent have felt at least once a presence in the room they where they are present, while 26.3% have even smelled an odor (foul or pleasant) without an apparent physical source.
Ninety clients surveyed have at least once witnessed a déjà vu experience. The incidence of telepathy is just as high. At least 90% were thinking of someone when he/she called immediately after their feeling, while 88% were about to speak out to their spouse or partner only to hear from them the very wording they were about to express.
More than two thirds feel that they have intuitive experiences, 23.2% think that they are very advanced intuitives. On the other end of the spectrum 10% of the people have never had an intuitive hunch. As far as precognition is concerned (N=204) 68.6% had precognitive experiences through dreams, 23.5% through waking visions and 11.3% through apparitions of dead relatives. One in four people have had at least once an out of body experience (OBE), while only three cases have had an NDE as recorded in the ICU.
Evil Eye is a concept that is not very well known in modern western societies. As stated by Wikipedia: “the evil eye is a curse or legend believed to be cast by a malevolent glare, usually given to a person when they are unaware”. However, even Socrates mentioned the power of the Evil Eye in antiquity.[2] At least half of this surveyed group are affected by it. On the other end, only 10% have never felt its effect.
I have adopted a question from the largest survey ever done by the SPR published in the nineteenth century Apparitions of the Living. The question is this: “Have you ever, when believing yourself to be completely awake, had a vivid impression of seeing or being touched by a living being or inanimate object, or of hearing a voice, which impression, so far as you could discover, was not due to any external physical cause?” (Gurney, E. et al, p.7 1888). One quarter of my clients answered positively on this question. That, to me, is a very significant percentage.
Many of the questions are not dealt with here because they are open ended and do not fit in the “yes or no” category or as appropriate multiple choices. Those questions contain very interesting details and material that would require much more space to publish and properly analyze.
Conclusion
I hope that our colleagues will find this input helpful as well as useful and that they will adopt it for use in their own practice. All things fluctuate and change with progress. Years ago, I had no questions on my questionnaire concerning tattoos, now I see that the tendency in younger ages is to mutilate their skin with all sorts of bizarre figures. As a result I modified my questionnaire to include three questions on tattoos. Who knows what the next fad will be? The aforementioned Dr. Poddarhose use of the online google form triggered my adoption of this practice, had a whole section on dietary habits. To my understanding all I needed to know instead was whether my clients are omnivorous, vegetarian, or vegan.
Maybe I am wrong, and she is right. I am looking forward to the time when EARTh will standardize this OIF so that all of us can use it and have more robust data to study.
[1] The experience of being hagged as found in Newfoundland tradition, then, may be summarized as follows: (1) awakening (or an experience preceding sleep);(2) hearing and/or seeing something coming into the room and approach the bed; (3) being pressed on the chest or strangled; (4) inability to move or cry out until either being brought out of the state by someone else or breaking through the feeling of paralysis on one’s own.” (Hufford 1982, p. 10-11)
[2] “My friend,” said Socrates, “do not be boastful, lest some evil eye put to rout the argument that is to come.” (Plato, Phaedo, 95b).
REFERENCES
Gurney, E., Myers, F., & Podmore, F. (1888). Phantasms of the living. London: Society for Psychic Research.
Hersen, M. & Van Hasselt, V. B. (2008). Basic interviewing: A practical guide for counselors and clinicians. Hove, Sussex: Psychology Press.
Hufford, D. (1982). The terror that comes in the night. An experience centered study of supernatural assault traditions. Philadelphia: University of Pennsylvania Press.
Kappas, J. (2001). Professional hypnotism manual. A practical approach for modern times. Van Nuys, CA: Panorama Publishing Company.
Kinsey, A., Pomeroy W., Martin C. (1948) Sexual behavior in the human male. Bloomington, IN: Indiana University Press.
Komianos, A. (2010). “Do we use intake forms, and standardized questionnaires?” Workshop presentation at the 2010 EARTh Annual Convention, Kleve, Germany.
Komianos, A. (2011). Rapid entity attachment release. Corfu: Hypnoscopesis Publishing.
Krippner, S., Bozgaran, F., & Percia de Carvalho, A. (2002). Extraordinary dreams and how to work with them. Albany, NY: State University of New York Press.
Papadatou-Pastou, M., Ntolka, E., Schmitz, J., Martin, M., Munafò, M. R., Ocklenburg, S., & Paracchini, S. (2020). Human handedness: A meta-analysis. Psychological Bulletin, 146(6), 481–524
Stevenson, I. (1971). The diagnostic interview. New York: Harper & Row.
Stevenson, I. (1997). Reincarnation and biology. Westport, CT: Praeger Publishing.