by Gunjan Y Trivedi and Riri G Trivedi

 Abstract – In this Project Completion Report, Gunjan and Riri Trivedi, co-founders of the Society for Energy & Emotions, Wellness Space, Ahmedabad, India share the research methods, procedures and outcomes of a research study that sought to explore the impacts and outcomes of regression therapy and self-hypnosis techniques as applied to generalised anxiety and associated depression. Their research study was funded and supported by the EARTh Research Committee. Before and after measurements were taken using the GAD-7 to assess levels of generalised anxiety disorder, and the Major Depression Inventory (MDI) to assess levels of depression. The research results indicated statistically significant reductions within both cohorts of study respondents – regression therapy (N-108) and self-hypnosis (N-25) – associated with the interventions utilised. Despite the high levels of anxiety experienced by the regression therapy cohort of study subjects, the significant positive results assessed and determined for those receiving regression therapy were achieved in only five sessions. Due to differences in presenting anxiety levels for both groups (the individuals in the regression therapy group had significantly higher anxiety levels than those who chose the self-regulation option via self-hypnosis) between-group comparison was not possible.
Abstract – In this Project Completion Report, Gunjan and Riri Trivedi, co-founders of the Society for Energy & Emotions, Wellness Space, Ahmedabad, India share the research methods, procedures and outcomes of a research study that sought to explore the impacts and outcomes of regression therapy and self-hypnosis techniques as applied to generalised anxiety and associated depression. Their research study was funded and supported by the EARTh Research Committee. Before and after measurements were taken using the GAD-7 to assess levels of generalised anxiety disorder, and the Major Depression Inventory (MDI) to assess levels of depression. The research results indicated statistically significant reductions within both cohorts of study respondents – regression therapy (N-108) and self-hypnosis (N-25) – associated with the interventions utilised. Despite the high levels of anxiety experienced by the regression therapy cohort of study subjects, the significant positive results assessed and determined for those receiving regression therapy were achieved in only five sessions. Due to differences in presenting anxiety levels for both groups (the individuals in the regression therapy group had significantly higher anxiety levels than those who chose the self-regulation option via self-hypnosis) between-group comparison was not possible.
Overview of The Study
Study Background
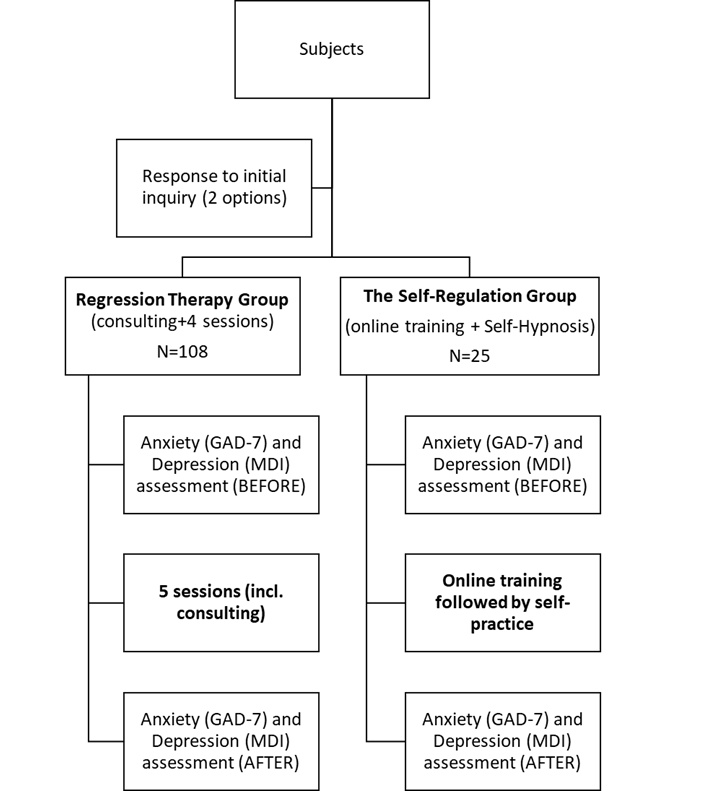
This study explored the impact of five regression therapy sessions (including one initial consultation session) on adults presenting with anxiety and associated depression. A choice was offered to study respondents to engage in regression therapy or undertake a self-regulation technique protocol. Those who elected to participate in the self-regulation cohort took part in a short training that utilised the SEE Protocol for self-hypnosis, and were also assessed for the impact on anxiety and depression levels before and after the intervention.
Study Aims, Questions and Hypothesis
The study aimed to understand the impact of two therapeutic interventions, regression therapy and self-hypnosis, on generalised anxiety. Whilst pre- and post-intervention levels of depression were measured, the primary focus of the study was the potential effects of the interventions upon anxiety. In seeking to conceptualise these aims, the following questions were framed:
- Is regression therapy an effective method to reduce anxiety (Generalised Anxiety Disorder or GAD) among Urban Adults?
- For individuals who do not choose the regression therapy intervention, is the self-hypnosis alternative an effective option to reduce anxiety (Generalised Anxiety Disorder or GAD) among Urban Adults?
The hypotheses are captured below:
- Regression therapy (total five sessions including consulting, max 75 mins each) effectively reduces anxiety levels for urban adults.
- Self-regulation training followed by two weeks of daily self-hypnosis practice (min 5 days/week) effectively reduces anxiety levels for urban adults.
Study Subjects
The study participants were recruited through word of mouth, social media and the Wellness Space website (Trivedi & Trivedi, n.d.). No paid advertising was done. The study participants were informed about the two intervention protocols (regression therapy and self-hypnosis) and selected one of the two options. Signed informed consent was taken from all participants.
Inclusion criteria for participation in the study: Urban adult individuals, aged between 18 to 60 years old, open to an online mode of intervention. Exclusion criteria for participation in the study: Individuals with a long-term (>15 years) psychiatric medical history or those who pursued both options.
Study Methods
All study subjects were provided with two intervention options:
- Regression Therapy Sessions – Personalised interventions that included one initial session of consultation and four therapy sessions (in a total of four weeks). The regression therapy interventions focused on regressing the subject to current life events, which carried an emotional charge with the aims of releasing the emotions from the body and reframing the event in the mind. This is known as ‘The Release Reframe Toolkit’ (See Table 1 below). One hundred and eight participants were involved in this intervention (N=108).
- Self-Hypnosis Protocol – Including 12-hours of online training (three hours per day over a four day training period) followed by two weeks of voluntary daily self-practice of the SEE Protocol for self-hypnosis – an evidenced-based 20-min long active meditation protocol (See Table 2 below) (G. Trivedi et al., 2020). There were twenty-five participants involved in this intervention (N=25).
Measurement Tools
The changes in anxiety and depression levels were evaluated for each group before and after the study interventions using the Generalised Anxiety Disorder (GAD-7) and Major Depression Inventory (MDI) self-assessment forms.
Conceptualisation and Modification of the Study
The study was conceptualised and modified several times with a clear focus on assessing and addressing generalised anxiety disorder. The original approach of the researchers (pre-COVID-19) involved conducting regression therapy sessions and training in self-hypnosis on a face-to-face basis.
However, within a context including growing levels of societal anxiety and depression, a variety of constraints associated with COVID-19, and a need to commence the project, the researchers decided that adaptations to the original intervention methods were necessary.
The researchers therefore moved towards the utilisation of virtual therapeutic interventions and trainings. Online individual therapy and online versions of training were offered, and individuals seeking support were able to choose individual therapy or simple self-regulation training involving the self-hypnosis protocol.
Of importance to note is that research in Cognitive Behavioural Therapy (CBT) indicated that the outcomes from online and face-to-face therapeutic interventions generally produce equivalent results (Axelsson et al., 2020; Carlbring et al., 2018).
Diagram of Study Design and Formation
Anxiety and Depression
A recent systematic review and meta-analysis among 63,439 individuals found that about one in three individuals have anxiety. The evidence also provides similar data for stress and depression (Salari et al., 2020). This is consistent with our experience at the Society for Energy & Emotions, Wellness Space Ahmedabad in India.
Anxiety is connected with constant worry or apprehension about future adverse events, often based on past experiences that impact various aspects of the mind and the body – ranging from hyper-arousal to inability to concentrate (Robinson et al., 2013). It is a response to a prolonged, unpredictable threat that involves the body, emotions and cognitive changes (e.g. focus or memory) (Grillon, 2008). Anxiety disorders are the most common forms of psychiatric disorders (Locke et al., 2015). Large numbers of individuals who seek psychiatric help have some level of anxiety even if they cannot articulate it. The examples include some form of internal agitation in the mind, and restlessness without acknowledging the nervousness accompanying the anxiety (Roy-Byrne, 2015; Thibaut, 2018).
Anxiety disorders are often accompanied by depressive disorders adding more risk to the overall health & well-being of the individual; Bandelow et al. (2017) found that major depression was highly correlated with all anxiety disorders in an extensive European survey. Anxiety disorders significantly impact the individual and the overall health care system due to their substantial social and economic consequences.
Anxiety is anticipatory and could consume many resources, leading to helplessness, withdrawal, and attentional difficulties. It is often associated with challenges related to emotional regulation and is known as the ailment of emotions.
Anxiety is caused by a failure to elect an adaptive response or address a maladaptive reaction to a stimulus, impacting the quality of life (Amstadter, 2008; Newman et al., 2013).
Anxiety is considered pathological when it arises in the absence of challenge or stress, when it is out of proportion to the challenge or stress in duration or severity when it results in significant distress and disrupts well-being, and when it results in psychological, social, occupational, biological, and other impairment (J. Trivedi & Gupta, 2010).
In short, the literature review indicates that anxiety causes a strong emotional regulation challenge, and these challenges are often connected with suppressed emotions related to past incidents (Mennin et al., 2005). Whilst there are varied psychotherapeutic and pharmacological treatments utilised to assist those suffering, the research indicates an important role for psychotherapy in treating anxiety and depression (Barkowski et al., 2020; Weitz et al., 2018). The importance of physical activity and stress management through relaxation techniques also helps in anxiety conditions (Bandelow et al., 2017; Ferreira-Vorkapic et al., 2018).
Given the role of past experiences and emotional suppression, this study explores whether releasing the emotional energy related to past incidents and reframing the issue using regression therapy methods could improve anxiety disorders.
Overview of Interventions
Regression Therapy Intervention
Regression therapy involves working with the challenges faced in the mind and the body, which have some emotional and energetic linkage to the events in the past. Common problems by subjects who seek help from regression therapists include relationship issues, anxiety, phobias, social challenges such as a lack of confidence, anger, relationship issues, unexplained body symptoms (e.g. migraine), addictions, sexual problems, eating disorders and so on (Tasso International, n.d.). These presenting problems may link with painful or traumatic events in the current life or past life.
Based on the brief description above, it is clear that regression therapy focuses on the emotions and energy associated with the specific incident(s) that occurred in the past that are traumatic and how they impact the physical body in the present – either manifesting as a physical or an emotional challenge.
While very effective, the researchers believe that regression therapy is somewhat limited to individuals who believe in it or those who have had exposure to its immense benefits. More evidence of its efficacy is needed to increase the share of regression therapy as a modality in complementary therapies. Medical professionals, the first point of contact for many individuals seeking help, may refer more easily when there is more evidence regarding the effectiveness of regression therapy interventions. This study focused on assessing anxiety levels and associated depression before and after regression therapy to understand how the sessions impacted the pre-assessed scores. One of the intentions for this structured study is to increase the evidence associated with regression therapy as an intervention.
Table 1 highlights the critical intervention strategies/methods and the specific techniques used during the regression therapy sessions. After an initial consultation session, all study participants in the regression therapy cohort engaged in four regression therapy sessions.
The GAD-7 and MDI assessments were completed before the initial consulting session and after completion of the four regression therapy sessions.
| Key intervention Strategies/Methods | Specific Techniques |
| 1. Regression into emotionally significant events | Using Bridges or Guided Imagery |
| 2. Release the emotional charge from the body and resolve any blocks in the mind and the body as necessary | Traditional Regression Therapy transformational techniques, Gestalt, Breathwork, Energy Exchange, Voice dialogue, Relationship drama |
| 3. Reframe in the mind | Perceptual Positioning, Anchoring, Reconsolidation of Traumatic Memory |
| 4. Integration and Future pacing | Gestalt, Anchoring and Guided Imagery |
Table 1 Key steps involved in Regression Therapy
Self-Hypnosis Intervention
The self-hypnosis intervention group attended a four-day training (three hours per day) that covered the importance of mind-body interventions in psychosomatic disorders, including anxiety and depression. The training also included a life-priority matrix to identify a future goal, the Emotional Freedom Technique (EFT) as an emergency emotional management tool, and the SEE Protocol for Self-Hypnosis (G. Trivedi et al., 2020).
The SEE Protocol for Self-Hypnosis is an evidence-based technique based on the yogic concept (a mind-body intervention) that helps in enhancing the quality of emotions (increases positive affect, decreases negative affect) and physiology (Heart Rate Variability). Weekly group calls were provided to this group after the training to facilitate a review session and answer questions, if any.
Table 2 below shows the key steps involved in the SEE Protocol for Self-Hypnosis.
| # | Activity | Description | Duration |
| 1 | Simple humming | Comfortable seating position, avoid if vertigo | 5 min |
| 2 | Coherent breathing | 10s (5 s inhalation and 5 s exhalation) as per the comfort focus on the heart centre | 5 min |
| 3 | Invoking positive emotions (e.g., gratitude and love) | Focus on the heart centre, maintain coherent breathing and invoke the emotions | 5 min |
| 4 | Guided imagery | Based on the prework of an identified goal. Invoke the state related to the goal | 5 min |
Table 2 Steps involved in the SEE Protocol for Self-Hypnosis
Research Assessment and Analysis
Table 3 below shows the essential measurement tools used for the study and examples of their appropriate usage and benefits:
| Measurement area | Type of measure | Examples (ease of use) | Outcome/Benefits |
| Generalised Anxiety Disorder | GAD-7 scale | Very useful and can differentiate versus the depression score. Provides good agreement between self-administration and interview scores | The GAD-7 is a useful and efficient tool for screening GAD and assessing its severity in clinical practice and research (Spitzer et al., 2006). |
| MDI Depression Index | MDI Survey | The MDI is a conservative instrument for diagnosing ICD-10 depression in a clinical setting (Konstantinidis et al., 2011; Nielsen et al., 2017). | More conservative versus the Beck Depression Inventory |
Table 3 Measurement tools used in the study
Research Results
The demographics (age, gender) and anxiety levels are captured below in Table 4 and Table 5. The data shows that most individuals, upon inquiry and follow-up, chose to pursue individual sessions through regression therapy (N=108). Given the differences in the profiles of the two groups based on the anxiety levels, a between-group comparison was not possible. After removing the dropouts (significantly high, >50% in the self-hypnosis group, very low, <15% in the regression therapy group, mainly due to an inability to complete four sessions in about a maximum of three weeks), the final sample size was 108 and 25, in regression therapy and self-hypnosis groups respectively.
Regression Therapy Group
| Gender | Count | Age | Anxiety Level (GAD-7 classification) |
| Female | 77 | 34.7-±9.6 | 13.3±6.6 (moderate) |
| Male | 31 | 32.8±8.9 | 14.5±6.3 (moderate) |
| Total | 108 | 34.1±9.4 | 13.6±6.5 (moderate) |
Table 4 Demographics of Regression Therapy Group
Self-Hypnosis Group
| Gender | Count | Age | Anxiety Level (GAD-7 classification) |
| Female | 17 | 39.4±8.5 | 7.8±5.8 (mild) |
| Male | 8 | 35.9±10.1 | 5.3±3.4 (none) |
| Total | 25 | 38.2±9.0 | 7.0±5.2 (mild) |
Table 5 Demographics of Self-Hypnosis group
Table 6 below shows before and after data on anxiety levels (as per the GAD-7 assessment) and depression levels (as per the MDI assessment) in the regression therapy group. Based on respective assessment surveys (Table 3), the classification of anxiety and depression levels indicate a “moderate” level. The reduction in anxiety levels for the regression therapy group was statistically significant, and similarly, the decrease in the depression levels were also statistically significant.
For readers not fully versed in statistical analysis, a p-value of 0.000 is statistically significant because it indicates 100% confidence about what is being tested i.e. in this case, regression therapy reduced anxiety and depression. This, therefore, rejects what is known as the null, that there is no difference.
| Type of measurement (Regression Therapy) | Before | After | p-value |
| Anxiety Level (GAD-7 classification) | 13.6±6.5 (moderate) | 6.5±4.5 (mild) | 0.000 (Statistically Significant) |
| Depression Level (MDI classification) | 27.4±11.9 (moderate) | 14.4±10.6 (none) | 0.000 (Statistically Significant) |
Table 6 Changes in Anxiety and Depression levels in Regression Therapy group
Table 7 below shows how the anxiety and depression levels decreased in those within the regression therapy group. The reduction for individuals with moderate and severe anxiety levels is also statistically significant and more pronounced (p <0.000). This is a significant outcome of the research, especially since any reduction in GAD-7 scores of more than four points is considered statistically significant (Bauer-Staeb et al., 2021).
The corresponding decrease in MDI (depression levels) for these individuals also adds to the importance of the findings, especially for moderate to severe anxiety level groups. Overall, for all groups in the table below, the average “after” scores of GAD and MDI are significantly below the cut-off of 10 and 20, respectively.
| Presenting level of anxiety (Before)
(Regression Therapy) |
GAD-7 before | GAD-7 After | MDI Before | MDI After | Sample size |
| 1. None | 3.6 | 3.5 | 13 | 7 | 10 |
| 2. Mild | 8.6 | 5.8 | 21 | 14 | 18 |
| 3. Moderate | 13.1 | 5.9 | 27 | 13 | 34 |
| 4. Severe | 18.2 | 7.9 | 34 | 17 | 46 |
| Grand Total | 13.6 | 6.5 | 27 | 14 | 108 |
Table 7 Reduction in anxiety as per presenting anxiety category in Regression Therapy group
Also see Figure 1 below which is a visual representation showing changes in anxiety and depression, as assessed and evidenced using GAD-7 and MDI pre and post intervention scores, within the regression therapy cohort of study participants:
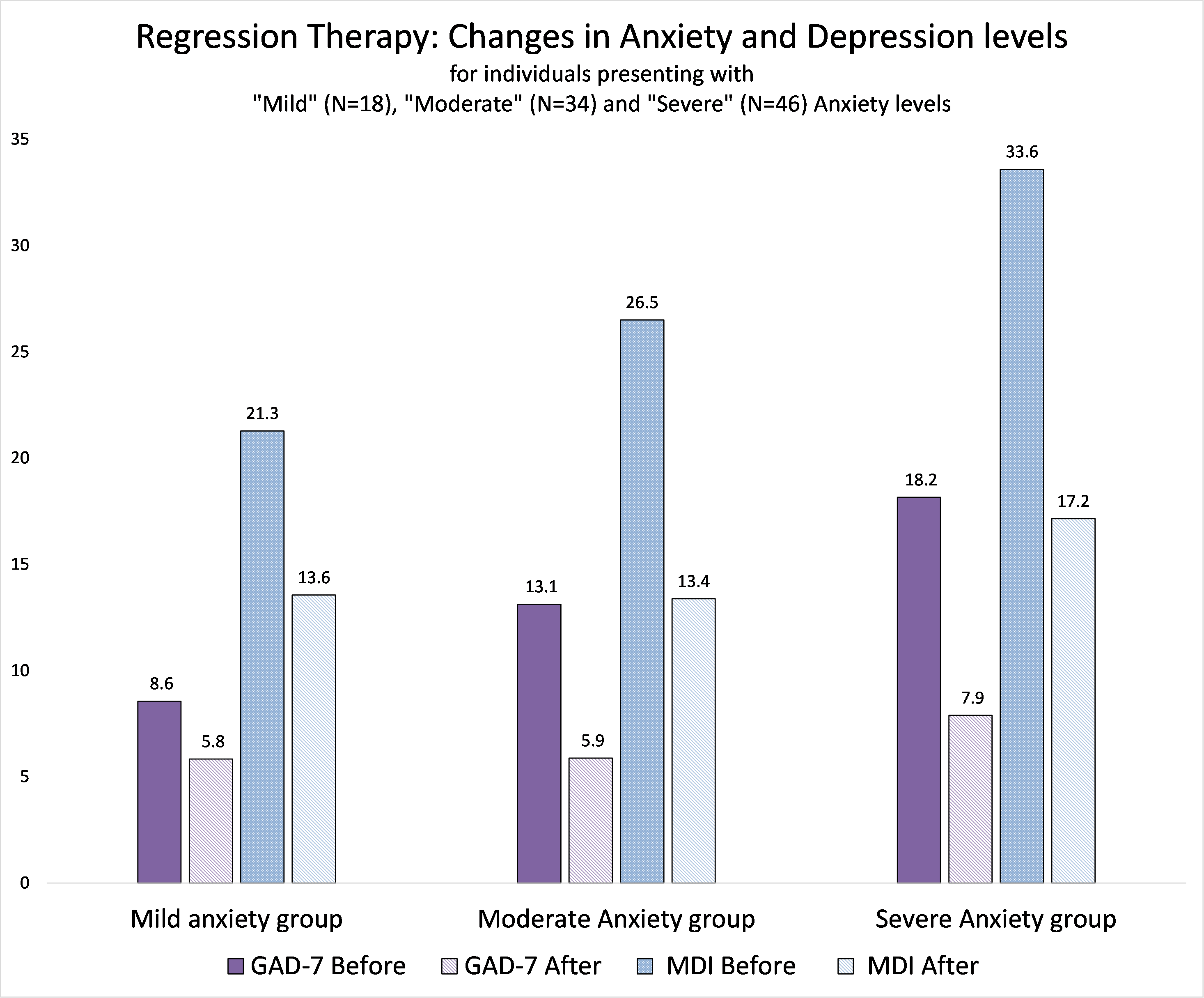
Figure 1 Visual showing changes in Anxiety and Depression levels (Regression Therapy group)
From an ethical perspective, participating in the self-hypnosis group provided an alternative to the individuals who wanted to work on their emotional and mental health while not pursuing regression therapy. For this group, the initial anxiety and depression levels of the individuals were not assessed as high, evidencing mild levels of anxiety as shown in Table 8. However, after learning the techniques and pursuing the self-hypnosis protocol for two weeks, this group also demonstrated a statistically significant reduction in anxiety and depression levels. For this group, the anxiety levels, as per GAD-7 classification are shown in Table 9. Given the sample size, especially in moderate and severe anxiety level groups (a total of 8 participants), the group comparison was not analysed.
| Type of measurement Self-Hypnosis | Before | After | p-value |
| Anxiety Level (GAD-7 classification) | 7.0±5.2
(mild) |
4.1±2.6 (none) | 0.001 (Statistically Significant) |
| Depression Level (MDI classification) | 13.4±7.8 (none) | 8.4±5.1 (none) | 0.000 (Statistically Significant) |
Table 8 Changes in Anxiety and Depression levels in the Self-Hypnosis group
| Anxiety Levels (GAD-7 classification)
Self-hypnosis |
GAD-7 Before | GAD-7 After | MDI Before | MDI After | Sample size |
| 1. None | 2.0 | 2.3 | 7.3 | 4.5 | 11 |
| 2. Mild | 7.7 | 4.5 | 13.3 | 11.0 | 6 |
| 3. Moderate Anxiety | 12.4 | 5.6 | 22.4 | 12.1 | 7 |
| 4. Severe Anxiety | 19.0 | 4.0 | 19.0 | 8.0 | 1 |
Table 9 Reduction in anxiety as per presenting anxiety category in Self-Hypnosis group
Overall, the results confirm that the intervention modalities provided to the participants, i.e. regression therapy and self-hypnosis, were effective in reducing anxiety levels. For both the groups, after the interventions, the depression levels also indicated a statistically significant reduction. Together, the results validate both research hypotheses.
Discussion
As per the researchers’ understanding and literature review, this work is one of the first research studies in the area of assessment and intervention pertaining to generalised anxiety disorder in association with regression therapy. Given the need for an ethical response to an inquiry on anxiety, each participant was provided with a second alternative to engage in a self-regulation protocol utilising self-hypnosis. Both intervention methods have demonstrated statistically significant reductions in anxiety and depression levels.
The reduction, specifically in moderate and severe (average) anxiety level groups, was very significant in the regression therapy intervention.
The psychometric assessment tool, the GAD-7, indicates that a score of about eight could be considered a cut-off for the survey, whilst some highlight a score of 10 (Johnson et al., 2019). Validated evidence indicates that any reduction of 3.7 to 4 points in the GAD-7 score is a minimal clinically significant difference (MCID) (Bauer-Staeb et al., 2021). This is applicable confirmation in relation to this research study.
Additionally, considering the existing classification (in relation to levels of anxiety) in Table 7 for the regression therapy group, it is prudent to focus on the moderate and severe levels of anxiety. For these groups (#3-Moderate Anxiety, #4-Severe Anxiety), the reduction of 7.2 and 10.3 after the Regression Therapy indicates statistically significant reductions and exceeds the criteria for clinically relevant differences between the before and after GAD-7 score.
Therefore, the data confirms that regression therapy sessions (total five, including consulting, over max one-month duration) can result in clinically significant reductions in anxiety levels based on the GAD-7 self-assessment. Finally, both groups’ average ‘after’ levels are below the GAD-7 cut-off levels of 10 (or even below a more aggressive eight). The corresponding reduction in MDI levels for each anxiety category was statistically significant and showed a statistically significant reduction. MDI, a self-administered form, is a valid and relevant tool to measure depression (Konstantinidis et al., 2011; Nielsen et al., 2017). For the current research, with a focus on anxiety, the MDI data provides an additional validation about the benefits of regression therapy as an intervention.
Study Limitations and Future Research
There are few limitations of the study. Firstly, the limited samples in the self-hypnosis group meant that comparison between methods was not possible. Secondly, the Adverse Childhood Experiences (ACE’s) research indicates that individuals with higher ACE scores are more likely to face mental health challenges.
Hence, classifying the incoming participants by their ACE score (High, Low) could detail the individual risk profile. Future work in this area could consider (a) the addition of sample size, especially of higher levels of anxiety for the self-hypnosis group, (b) understanding the effectiveness of regression therapy variations in the outcome for various demographics (age, profession, gender, ACE level). Future research could also explore how regression therapy could help improve sleep quality and enhance the overall well-being of an individual.
Conclusions
Study outcomes indicated a statistically significant reduction in anxiety and depression levels for both groups. Therefore validating the effectiveness of regression therapy and self-hypnosis as interventions. The findings show that regression therapy sessions significantly reduced anxiety and depression levels among participants in just five sessions – even when the participants had high levels of anxiety before the therapy started. Additionally, in terms of the regression therapy intervention, the reductions in anxiety levels within the assessed moderate and severe classifications of anxiety were very significant. This may indicate heightened benefits in the application of regression therapy to client presentations of moderate and severe anxiety, and perhaps from a practitioner’s perspective, indicate that it may be prudent to focus on these levels of anxiety within the field of regression therapy.
Acknowledgements
The authors wish to acknowledge the role of Bhumika Sheth, Client Manager, Wellness Space, Ahmedabad, for her role in providing the framework for both of the intervention options to the participants.
The authors also wish to acknowledge the overall guidance from Dr S Kathirvel (Associate Professor, School of Community Medicine and Public Health, PGI Chandigarh) in terms of structuring the research methodology and framework at the Society for Energy & Emotions, Wellness Space, Ahmedabad, India.
The authors also wish to acknowledge the help and support from Paula Fenn and the Research Committee, Earth Association for Regression Therapy (EARTh), for ongoing counsel from the conception to the closing stages of this project. EARTh provided partial funding for this study in 2020.
References
Amstadter, A. (2008). Emotion regulation and anxiety disorders. Journal of Anxiety Disorders, 22(2), 211–221.
Axelsson, E., Andersson, E., Ljótsson, B., Björkander, D., Hedman-Lagerlöf, M., & Hedman-Lagerlöf, E. (2020). Effect of Internet vs Face-to-Face Cognitive Behaviour Therapy for Health Anxiety: A randomised Noninferiority Clinical Trial. JAMA Psychiatry, 77(9), 915. https://doi.org/10.1001/jamapsychiatry.2020.0940
Bandelow, B., Michaelis, S., & Wedekind, D. (2017). Treatment of anxiety disorders. Dialogues in Clinical Neuroscience, 19(2), 93–107.
Barkowski, S., Schwartze, D., Strauss, B., Burlingame, G. M., & Rosendahl, J. (2020). Efficacy of group psychotherapy for anxiety disorders: A systematic review and meta-analysis. Psychotherapy Research: Journal of the Society for Psychotherapy Research, 30(8), 965–982. https://doi.org/10.1080/10503307.2020.1729440
Bauer-Staeb, C., Kounali, D.-Z., Welton, N. J., Griffith, E., Wiles, N. J., Lewis, G., Faraway, J. J., & Button, K. S. (2021). Effective dose 50 method as the minimal clinically important difference: Evidence from depression trials. Journal of Clinical Epidemiology, 137, 200–208. https://doi.org/10.1016/j.jclinepi.2021.04.002
Carlbring, P., Andersson, G., Cuijpers, P., Riper, H., & Hedman-Lagerlöf, E. (2018). Internet-based vs. face-to-face cognitive behaviour therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cognitive Behaviour Therapy, 47(1), 1–18. https://doi.org/10.1080/16506073.2017.1401115
Ferreira-Vorkapic, C., Borba-Pinheiro, C. J., Marchioro, M., & Santana, D. (2018). The Impact of Yoga Nidra and Seated Meditation on the Mental Health of College Professors. International Journal of Yoga, 11(3), 215–223. https://doi.org/10.4103/ijoy.IJOY_57_17
Grillon, C. (2008). Models and mechanisms of anxiety: Evidence from startle studies. Psychopharmacology, 199(3), 421–437. https://doi.org/10.1007/s00213-007-1019-1
Johnson, S. U., Ulvenes, P. G., Øktedalen, T., & Hoffart, A. (2019). Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample. Frontiers in Psychology, 10, 1713. https://doi.org/10.3389/fpsyg.2019.01713
Konstantinidis, A., Martiny, K., Bech, P., & Kasper, S. (2011). A comparison of the Major Depression Inventory (MDI) and the Beck Depression Inventory (BDI) in severely depressed patients. International Journal of Psychiatry in Clinical Practice, 15(1), 56–61. https://doi.org/10.3109/13651501.2010.507870
Locke, A. B., Kirst, N., & Shultz, C. G. (2015). Diagnosis and management of generalised anxiety disorder and panic disorder in adults. American Family Physician, 91(9), 617–624.
Mennin, D. S., Heimberg, R. G., Turk, C. L., & Fresco, D. M. (2005). Preliminary evidence for an emotion dysregulation model of generalised anxiety disorder. Behaviour Research and Therapy, 43(10), 1281–1310.
Newman, M. G., Llera, S. J., Erickson, T. M., Przeworski, A., & Castonguay, L. G. (2013). Worry and generalised anxiety disorder: A review and theoretical synthesis of evidence on nature, etiology, mechanisms, and treatment. Annual Review of Clinical Psychology, 9, 275–297.
Nielsen, M. G., Ørnbøl, E., Bech, P., Vestergaard, M., & Christensen, K. S. (2017). The criterion validity of the web-based Major Depression Inventory when used on clinical suspicion of depression in primary care. Clinical Epidemiology, 9, 355–365. https://doi.org/10.2147/CLEP.S132913
Robinson, O. J., Vytal, K., Cornwell, B. R., & Grillon, C. (2013). The impact of anxiety upon cognition: Perspectives from human threat of shock studies. Frontiers in Human Neuroscience, 7. https://doi.org/10.3389/fnhum.2013.00203
Roy-Byrne, P. (2015). Treatment-refractory anxiety; definition, risk factors, and treatment challenges. Dialogues in Clinical Neuroscience, 17(2), 191–206.
Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S., & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalisation and Health, 16(1), 57. https://doi.org/10.1186/s12992-020-00589-w
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A Brief Measure for Assessing Generalised Anxiety Disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092. https://doi.org/10.1001/archinte.166.10.1092
Tasso International. (n.d). Regression therapy for what kind of problems. https://www.tassointernational.com/regression-therapy/regression-therapy-for-what-kind-of-problems
Thibaut, F. (2018). The mind-body Cartesian dualism and psychiatry. Dialogues in Clinical Neuroscience, 20(1), 3.
Trivedi, G., Patel, V., Shah, M., Dhok, M., & Bhoyania, K. (2020). Comparative study of the impact of active meditation protocol and silence meditation on heart rate variability and mood in women. International Journal of Yoga, 13(3), 255–260. https://doi.org/10.4103/ijoy.IJOY_18_20
Trivedi, J., & Gupta, P. (2010). An overview of Indian research in anxiety disorders. Indian Journal of Psychiatry, 52(7), 210. https://doi.org/10.4103/0019-5545.69234
Trivedi, G.Y., & Trivedi, R.G. (n.d.). Wellness space: Transforming individuals and teams. https://wellness-space.net/about-us/
Weitz, E., Kleiboer, A., van Straten, A., & Cuijpers, P. (2018). The effects of psychotherapy for depression on anxiety symptoms: A meta-analysis. Psychological Medicine, 48(13), 2140–2152. https://doi.org/10.1017/S0033291717003622