by Marc Van Hecke DO, BSc
 Abstract: Highly Sensitive Persons (HSP) suffer from the many sensory stimuli that come into their system. Elaine Aron writes in her book “the Highly Sensitive Person” that 20 % of people are born with a highly sensitive nervous system and that’s why they suffer so much. Is this true? Or is hypersensitivity the result of trauma, occurred in early childhood, prenatal, or even has his roots in previous lives? Are the psychoenergetic residues of trauma the cause of a disturbance of the nervous system? This work tries, by focusing on the most sensitive sense of each individual, to regress the client and heal the trauma situation linked to the hypersensitivity. Ten HSP estimated the nuisance they had from their most sensitive sense on a VAS (visual analogue scale). They were submitted to two regressions in a period of two to three weeks. Two weeks after the second session they evaluated it again. Our hypothesis was: ‘Regression therapy can diminish the inconvenient hypersensitivity of the senses in HSP and so can improve the quality of life of HSP’. The data were statistically analyzed and with the Paired Student T-test the results were statistically significant at p = 0.0014. The null-hypothesis could be rejected. We conclude that regression therapy may reduce the nuisance that HSP have from their state of hypersensitivity.
Abstract: Highly Sensitive Persons (HSP) suffer from the many sensory stimuli that come into their system. Elaine Aron writes in her book “the Highly Sensitive Person” that 20 % of people are born with a highly sensitive nervous system and that’s why they suffer so much. Is this true? Or is hypersensitivity the result of trauma, occurred in early childhood, prenatal, or even has his roots in previous lives? Are the psychoenergetic residues of trauma the cause of a disturbance of the nervous system? This work tries, by focusing on the most sensitive sense of each individual, to regress the client and heal the trauma situation linked to the hypersensitivity. Ten HSP estimated the nuisance they had from their most sensitive sense on a VAS (visual analogue scale). They were submitted to two regressions in a period of two to three weeks. Two weeks after the second session they evaluated it again. Our hypothesis was: ‘Regression therapy can diminish the inconvenient hypersensitivity of the senses in HSP and so can improve the quality of life of HSP’. The data were statistically analyzed and with the Paired Student T-test the results were statistically significant at p = 0.0014. The null-hypothesis could be rejected. We conclude that regression therapy may reduce the nuisance that HSP have from their state of hypersensitivity.
Remarkably, all subjects came to early childhood or prenatal traumas. The most common cause was a poor or traumatic relationship with the mother. None of the subjects went back to a previous life.
Introduction
For many years now high sensitivity is well known. Among others, Elaine N. Aron is the author of several books on high sensitivity. Many people recognized themselves in the description of high sensitivity in her books. They must have been relieved to realize that there was a name, a diagnosis for the symptoms they suffered from. As in many cases in medicine, patients are temporarily alleviated by diagnosis, as they think: “they know what I am suffering”. The next question is what to do about it. For HSP the answer is disappointing: learn to live with it, use the possibilities in a positive way, feel and respect your borders.
What is a High Sensitive Person?
Our nervous system has to deal with many stimuli. Through all our senses much information enters our body, which allows us to move and act in this world. We hear, see, taste, smell and feel around us and absorb whatever, in one way or another, is important for us. Besides, we process stimuli of our body: hunger, thirst, pain, pressure, or simply how our clothes itch. These senses give us information about ourselves. We handle a huge amount of stimuli to survive in the modern, quickly changing world.
Highly sensitive people cannot process that huge number of stimuli, they are already overwhelmed by few stimuli. Maybe information that enters has a different meaning, maybe they cannot screen or filter it or maybe their nervous system can only handle fewer stimuli.
According to Elaine Aron, a more sensitive nervous system is the cause of high sensitivity. Highly sensitive persons are overwhelmed by an amount of information that others consider normal. This is arduous and hinders them in normal functioning. Aron assumes that about 20% of people are born with a more sensitive nervous system and they are stuck with it. They have to learn to live with it and try to turn to good account its inconveniences. The fact that most HSP report that they suffer from it from an early age confirms for Aron that they are born with it.
I doubted this assumption. High sensitivity may not be a characteristic we are born with; it may be acquired. I wanted to research this further and find the answers to two questions: What causes HSP? And what can we do about it?
As we know, the autonomous nervous system (ANS) changes our senses in dangerous situations. The pupils dilate, the hearing is finer, the skin more sensitive, blood pressure higher, the heartbeat faster and adrenaline increases: the whole body goes into alert mode. This helps to fight or to flee in threatening situations. And of course, dangerous situations can be situated in early childhood, birth, prenatal or even in past lives. In danger, the alert mode is switched on and if not processed by action (like in freezing or blocking) stays on, annoying the subject.
In the evolution of the brain, we can distinguish three levels: the reptilian, the mammal and the human brain. We may name them ‘instinctive’, ‘reactive’ and ‘creative’ brain. Strangely enough, simpler animals can switch of this alert mode when danger has passed. For one reason or another, for the more sophisticated human brain it seems very difficult to turn off this mode. If we can work on the causes that brought the nervous system in alert mode, we probably can switch off this mode and senses will become peaceful and tranquil. For HSP this means that they would stop suffering from an overload of stimuli and would deal with what is coming in: being less bothered with noise or light, etc. And even if those are abundant, they would be able to handle it and draw borders. They would not be overwhelmed anymore. In HSP it seems as if all senses are open, in alert mode, as if they – or a part of them – are stuck, frozen in a traumatic event.
If high sensitivity is the result of traumatic experiences and we can work out the residues with regression therapy, the burden of high sensitivity must decrease or disappear after therapy.
Research method
I wanted to find out if high sensitivity has a reason, an origin. If so, and if this origin can be healed, it should improve the well-being of the subjects and reduce the negative effects of the sensitivity.
So I searched 10 highly sensitive persons to undergo 2 regression sessions within two or three weeks, on their most sensitive (bothering) sense.
I found them by asking HSP candidates for research in my practice as an osteopath, by distributing flyers about my research in the Flemish Association for HSP, and through an announce in a popular magazine. Forty people reacted: two male and 38 female.
I recruited them in the order they came in. Some of the candidates refused or were not able to do the travel and some thought it was only an inquiry and didn’t want to do sessions, so they were excluded. I excluded those taking anti depressants, and those younger than 18 or over 65 years.
Once I had ten people who met the criteria, I put the others in stand-by, in case some wouldn’t show up or wouldn’t complete the two sessions. They filled in an information form, underwent two sessions regression therapy and again after a fortnight filled in another form to evaluate the result. In this information form they gave a VAS-score (visual analog scale) on their most bothering sensitivity. Two weeks after the second treatment they gave again a VAS score on the same issue. We also asked them to write down some impressions about the treatment and the result. The results were statistically analyzed.
We also looked at similarities in the sessions on the origin of their high sensitivity.
Null-hypothesis:
- Regression therapy does not diminish the bothering hypersensitivity of the Highly Sensitive Persons.
- Regression therapy cannot improve the quality of life of Highly Sensitive Persons.
Subjects and methods
They where all women between 26 and 53 years old: 2 in their fifties, 5 in their forties, 2 in their thirties and one woman of 27 years old.
Two men who signed up where not selected because one couldn’t make the trip to the practice and the other had too many other ailments, so the HSP diagnosis was not clear.
We may wonder if this is a general distribution of HSP: 5% men and 95% women. We didn’t investigate this further.
Many subjects had other diagnoses as well:
- 4 candidates where also diagnosed with fibromyalgia
- 4 also with chronic fatigue syndrome
- 2 with depression and another 2 had this diagnosis in the past
- 2 with burnout
- 1 with spasticity disorder: tightness or increased muscle tone.
The presence of those many other syndromes makes the diagnosis of HSP rather equivocal. (And the other diagnoses as well.)
In this article we don’t discuss individual candidates. We only mention some similarities and some ways of working to give an impression of what we encountered.
All candidates manifest multiple hypersensitive senses, but we asked them to choose the most sensitive. In the list, the marks are the number of the candidate.
Seeing: test subject 1 – 4 – 8 – 10
Hearing: test subject 5 – 6 – 9
Feeling: test subject 7
Other: test subject 2 -3 (6th sense? Sensibility for emotion and moods of others, even if not present)
No candidates gave taste or smell as their most sensitive sense.
The improvement of bothering hypersensitivity is shown by the P-value for paired student t-test: significant: value 0.0014.
The values ‘before’ and ‘after’ are shown in the box plot A.
Used bridge and induction
Imaginary bridge: 3 – 5 – 6 – 8
Personification: 2 – 4 – 6 – 7 – 9 – 9 – 10
Aura exploration: 1 – 2 – 3 – 4 – 5 – 7 – 8 – 10
Somatic + Emotional bridge: S + E: 1
Personification and aura exploration were the most often chosen methods for beginning the regression, as at the start of the therapy the symptoms were not present. A few times the imaginary bridge was used because the candidates remembered clearly the situation that triggered the sensitivity. Only once S + E was used because the somatic charge was distinctly present at the start of the session.
Proper techniques were used at the moments they were required. Sometimes associative, sometimes dissociative. Postulates were defused and inner children seen, healed and integrated. Attachments, when present, were removed after energetic balancing. Results were anchored verbally or physically or by future pace. Only once a past life came by, but it appeared to belong to the mother and was properly detached. Physical, emotional and mental charges were dealt with and released.
Analysis
The data were analyzed using SAS (Statistical Analysis System), version 9.1.2, a powerful software package for the manipulation, analysis and presentation of data.
VAS scores table
| Candidate | Score before | Score after 2 regressions |
| 1 | 9 | 3 |
| 2 | 9 | 3.5 |
| 3 | 10 | 6.5 |
| 4 | 10 | 10 |
| 5 | 9 | 6 |
| 6 | 10 | 8 |
| 7 | 6 | 6 |
| 8 | 8 | 3 |
| 9 | 10 | 4 |
| 10 | 8 | 6 |
VAS scores diagram

Table of statistical data and results of the research
| Score | Score before | Score after | Difference |
| Mean | 8.900 | 5.600 | -3.300 |
| Median (Q2 = P50) | 9.000 | 6.000 | -3.250 |
| N (non-missing data) | 10 | 10 | 10 |
| N (missing data) | 0 | 0 | 0 |
| SD – Standard Deviation | 1.2867 | 2.2828 | 2.2998 |
| SE – Standard Error of the mean | 0.4069 | 0.7219 | 0.7272 |
| Minimum | 6.00 | 3.00 | -6.00 |
| 10th percentile (= P10) | 7.000 | 3.000 | -6.000 |
| Lower quartile (Q1 = P25) | 8.000 | 3.500 | -5.500 |
| Upper quartile (Q3 = P75) | 10.000 | 6.500 | -2.000 |
| 90th percentile (= P90) | 10.000 | 9.000 | 0.000 |
| Maximum | 10.00 | 10.00 | 0.00 |
| Lower limit 95% CI for mean | 8.103 | 4.185 | -4.725 |
| Upper limit 95% CI for mean | 9.697 | 7.015 | -1.875 |
| P-value for normality (Shapiro-Wilk test) | 0.0285 | 0.3143 | 0.2340 |
| P-value for Wilcoxon Signed Rank test | 0.0020 | 0.0020 | 0.0078 |
| P-value for Paired Student t-test | <.0001 | <.0001 | 0.0014 |
Out of the P-value for normality (Shapiro-Wilk test) we can decide that the VAS-scores of the subjects show a normal distribution or Gaussian curve. This validates the Paired Student t-test for this population and gives a probability for the null-hypothesis of 0.0014. The null-hypothesis can be rejected when this is smaller than 0,05, which is the case.
Box plot A: score ‘before’ (red) and ‘after’ (green) treatment.

Box plot B of mean differences between ‘before’ and ‘after’.
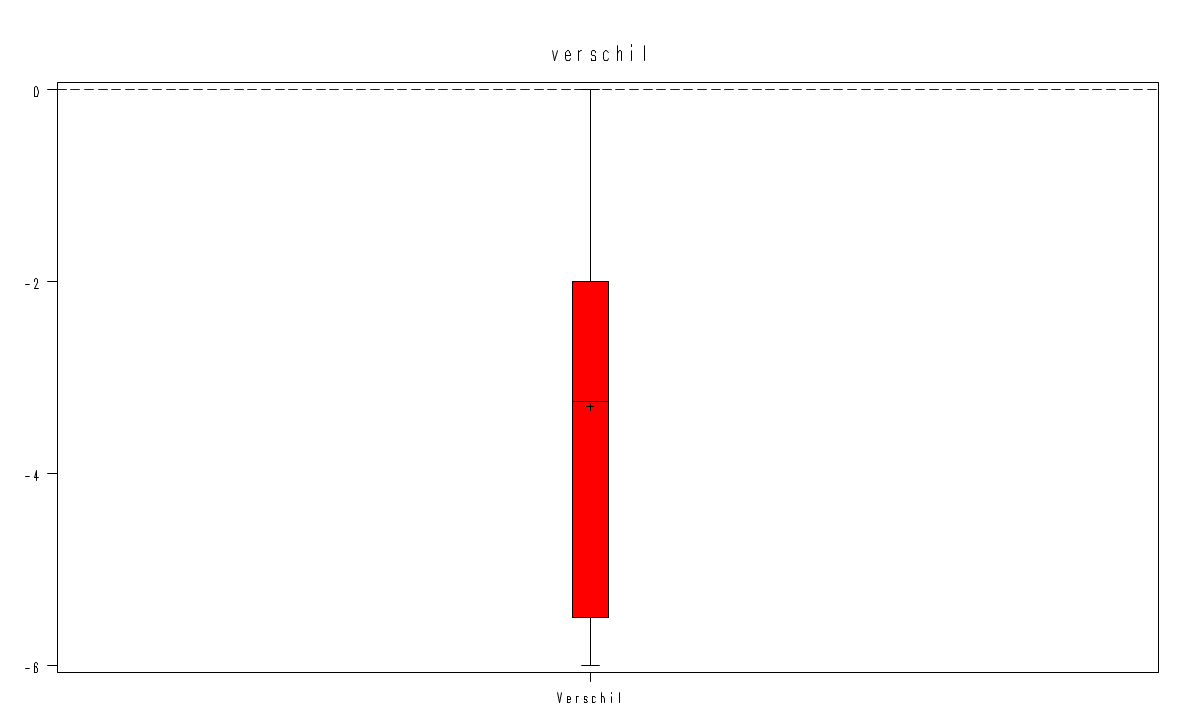
The smallest decrease is zero and the highest is 6. The mean difference is -3,3 and most of them are located between -2 (upper quartile Q3 = P75) and -5,5 (lower quartile Q1 = P25)
The mean difference ‘before’ and ‘after’ is -3,3 with a lower limit 95% CI for mean -4,725 and the upper limit 95% CI for mean -1,875. In other words 95% of the clients are in between those marks. Those marks are negative which means that no worsening can be expected for 95% of the cases.
The null-hypothesis can be rejected, because the P-value for the Paired Student t-test is less than 0,05 namely 0.0014. In other words, regression therapy can diminish inconvenient hypersensitivity. It can improve the quality of life as shown by the reactions of the subjects.
Conclusions
Experiences in the current life seem to be the origin of the hyper sensibility. Within these two sessions, nobody went back to a past life to find the cause. Despite the excellent improvements after regression, nobody goes to ‘zero’ irritation. We may wonder if that would be possible. Maybe after more sessions. Another question is: would we reach past lives when we did more sessions on the issue? May be, but at least it wasn’t necessary to reach significant improvements.
In two out of ten test subjects there was no improvement. With one we didn’t get in the issue, no trance. The other one admitted afterwards that she felt better, but didn’t show that in her marks (about skin sensitivity and rash).
Out of ten subjects eight go to childhood experiences where the mother is involved! Two where mother and father is involved.
Two candidates had to defend themselves against a raging mother: one was almost asphyxiated, and the other almost drowned! They were not accepted as child and they sensed that even before birth.
Four times, children failed to catch the attention of the mother.
Two children couldn’t be child-like because they had to take responsibilities for mother or father (parentification).
Three times we found an attachment: a grandmother, a father, and an apparent extra-terrestrial, but they seemed only indirectly involved in the hypersensitivity.
Mostly insight and understanding are the results of the sessions.
Some reactions of the test subjects
- There is more clarity towards several complaints. I can take more distance and I am less vulnerable.
- My headaches improved much, I am less disturbed by noises and the eczema in my neck improved.
- I can make better choices, put things more in perspective, can persevere and choose for myself.
- Comments of others don’t bother me anymore, I can protect myself. There is more apprehension: I need more contact with my belly-feeling to be stronger, to live.
- It was a special experience.
- The sessions gave me my desire in life back. I became calmer and the pain in my belly has gone (loneliness was stored there). I can smell again and am less afraid
- It’s easier to draw borders. It is a different way of working than normal psychotherapy.
- Regression therapy was an unusual experience for me. Rather arduous, but the insights I got about my personality were enlightening. I feel more tranquil and can leave my problems behind. I know better now what I want and like.
- A dormant stress has gone. This therapy has exposed certain things so I can better understand some disturbances in myself. I changed for the better.
- I am more peaceful, less rushed. I am more untroubled, calm, less stress
- I got some insights, understand myself. It is an enrichment and I can make better choices.
Candidates admit, and that’s confirmed by the statistics, that they suffer less from the hypersensitivity. Two candidates say they are more sensitive, but suffer less. This can imply that indeed they had a more sensitive nervous system that was overloaded.
Anyway, the results show that the hypersensitivity diminished after the treatment. The bothering feelings fade away after regression therapy. The question remains if the nervous system of HSP is more sensitive than in other people. It seems hardly relevant: after regression therapy they suffer less.
Suggestions for further research
It could be interesting to do more sessions and see if the VAS score reaches zero.
It should be worthwhile to treat more candidates to see if the results are always so auspicious.
By doing more sessions with more candidates, the interpretation of the cause can be refined. Now the mother’s relationship is the central issue, but what else could be aggravating circumstances?
More investigation should clear up the matter if HSP have a more sensitive nervous system or not. I think the so-called HSP live more aware, maybe ancient souls, and consequently they experience the disturbances of trauma more intensive and consciously than other people.
Nowhere in literature could I find articles concerning treatment of the causes of HSP. What I did find is: survival tips or tools and coaching to switch ‘highly sensitive people’ into ‘happy sensitive people.
References
Aron, E. N. (1996). The highly sensitive person. Carol Publishing group, ISBN: 0-553-06218-2
Aron, N. E. (1999). The highly sensitive person’s workbook. New York: Broadway books. ISBN 0-7679-0337-4
Bosch I. (2007). PRI: Past reality integration; rediscovering the true elf. (rev. ed.) ISBN: 90-807-0491-1
Herman, J. L. (1997). Trauma and recovery. Basic Book. ISBN 0-465-08730-2
Levine, P. A. (1997). Waking the tiger, healing trauma. Berkely, CA: North Atlantic Books. 1-55643-233-X
Marletta-Hart, S. (2000). Voluit leven met hooggevoeligheid, (Living Completely with High Sensitivity). Ten Have. ISBN 978 90 259 5671 4 / nur 770/728
Ten Dam, H. (1996). Deep healing. Tasso Publishing. ISBN 9789075568028
Van Cranenburgh, B. (1991). Schema’s fysiologie. (Diagrams of Physiology). De tijdstroom. ISBN 90-352-1419-6
http://en.wikipedia.org/wiki/Highly – sensitive – person