Past-life Regression Therapy (PLRT) applied in the treatment of patients diagnosed with insomnia
Dr. Bistrich Bibiana (MD) and therapists Ana Lucía Monzón, Edith Zas, Fabiola Zavalla Guerrero, Florencia del Signore.
Abstract: The specialists involved in this research decided to investigate the possibly beneficial effects of past-life regression therapy sessions on insomnia. The present study researches the effects of this therapy on insomnia patients. Thirty patients with insomnia did three past-life regression therapy sessions. After several months, significant changes in their symptoms were observed. We conclude that the use of transpersonal therapy helps to reduce and control the symptoms of insomnia.
Introduction: According to our own medical experience registered in medical records from previous years and prior to the present study, together with the increase in consultations for cases of insomnia in the last two years, the specialists who participated in this research have decided to further investigate in detail the effects (tentatively considered to be beneficial) of the past-life regression therapy sessions for patients that suffer from this condition.
According to the information gathered during the bibliographic research, it has been determined that insomnia is a very common pathology frequently seen among people in general. It is estimated that between 10 and 15 % of the adult population suffers from chronic insomnia, and that between 25 and 35 percent of adults have suffered temporary or occasional insomnia after undergoing stressful situations.
It has been noted that although the conventional treatments used nowadays help to reduce the symptoms of such pathology, once the medication or treatment provided at first (as the core medical measure) wears off, the same symptoms reappear. Therefore, it has been suggested that the use of an integrative approach as part of the therapeutic repertoire, together with the main medical treatment chosen, in which the whole being is considered and treated in an integral manner. Considering the human soul as an essential and vital part of the whole individual being treated, it has been determined that it is appropriate and relevant to address the main symptoms with the transpersonal approach offered by past-life regression therapy.
Clinical cases of patients who arrived at our facilities in search of medical assistance to treat their insomnia improved considerably after working with past-life regression therapy sessions. There were even some patients who reported that their symptoms of insomnia had disappeared completely. Therefore, some important questions arise: Is past-life regression therapy really effective when treating insomnia? Can it be considered a valid option to be integrated into the healing process of our patients who come to us for help?
With these considerations in mind, the Pilot Analytic and Prospective Clinical study has been designed to determine if past-life regression therapy can be considered a tool for treating patients clinically diagnosed with insomnia.
During the course of this study, Transpersonal Therapy was defined as the kind of therapy that helps an individual connect with his or her own identity. In its literal translation, the term transpersonal means “beyond the person himself or herself.” Thus, therapy in transpersonal psychology is designed to get to the deepest realms of our being. Finally, therapy is defined as that branch of medicine focused on describing several illnesses and working on the treatment itself. Basically, therapy is defined as the branch of medicine that describes illnesses and develops treatments.
Sleep disorder has been defined as a disorder that affects the normal sleep rhythm (wakefulness or state of vigilance), according to the Diagnostic and Statistical Manual of Mental Disorders. Diagnose Criteria DSM-5 780.52 (G47.00)
Method and resources:
A total of 30 patients between the ages of 25 and 53 (average age of 33.4) participated voluntary in the study (23 females and 6 males). All of them were already diagnosed with insomnia before the present study. Fifty percent (15 patients) were receiving medical treatment with benzodiazepines. Thirty percent (9 patients) did some type of meditation to help them fall asleep.
Inclusion criteria:
Males and females who have been diagnosed with insomnia by a physician, with or without any allopathic-based treatment between 18 and 65 years old. Of any ethnicity and socioeconomic level. Any educational level. Spanish-speaking.
Exclusion criteria:
Men and women who claim to suffer from insomnia but have not been properly diagnosed by a physician. Patients under the age of 18 and older than 65. Patients with other kinds of known psychiatric or neurological pathologies. Patients with disorders or syndromes that reduce their reading comprehension are less likely to understand the tasks or instructions given. Patients addicted to illegal drugs (according to Argentina’s legislation). People who, for whatever reason, could not travel to the clinic, thus excluding online work.
The present study included attention centres in Santiago de Chile (Chile), Ciudad Autónoma de Buenos Aires, Adrogué, Rafaela (Argentina), and Trecate (Italy). Moreover, five therapists in this study were trained specifically following the technique created by Dr. Cabouli.
Every patient who participated in this study was duly informed by the therapist in charge of the terms and conditions of the present research. Each patient was given and explained in detail the “informed written consent” based on the guidelines established by the World Health Organization (WHO).
Each patient was asked to complete an initial questionnaire (see grid below) to record the symptoms presented and their frequency and intensity before the first past-life regression therapy session. The same grid had to be completed after the last session. This was done in order to document any changes in the parameters measured.
Each participant in this study committed themselves to continuing with their regular medical examinations, as well as informing the researcher of any kind of change (subjective or objective) in the symptoms or medication given by their primary care physician that might have been previously indicated.
Three regression sessions of 70 to 90 minutes each (the average of a 76-minute session) were conducted in person using Dr. Cabouli’s method. Said method consists of transpersonal work through the expansion of consciousness. To achieve this, it is necessary to deepen the analysis of the symptom that the patient refers to at the time of consultation. This technique does not use clinical hypnosis, in fact, it involves allowing the patient to experience an expanded state of awareness.
consciousness that helps him/her to detect details which had never been perceived before, and then to establish its resemblance to an event. This generally responds to an experience excluded from the patient’s consciousness that, in turn, is the original cause of the clinical manifestation and the reason for which he/she seeks the professional’s opinion and help. After this experience – which is generally not part of the person’s biography – arises and manifests itself, the therapist accompanies the person who is performing the regression exercise, in order to complete it, i.e., to reach the end of it. Once the exercise is fully completed, a brief therapeutic intervention is conducted following the foreseen protocol. This is the moment in which the patient makes a kind of closure of the Gestalt. Finally, a harmonization is performed in order to facilitate the return to the patient’s usual state of consciousness.
The period between sessions was two weeks until the total number of sessions was reached. After a month, the researcher contacted the patient again to ask him to answer the survey carried out on day one. The follow-up of the study was completed two months after the beginning of the study.
Grid used: The following grid was completed on day 1, at the beginning of the study, during the first interview, and before session 1. It was completed again on day 60, when the follow-up control was carried out to document what happened after the three regression sessions.
| A | B | C | D | E | ||
| N | Symptom | Always | Frequently
(Specify how often) |
Regularly
(Specify how often) |
Rarely (Specify how often | Never |
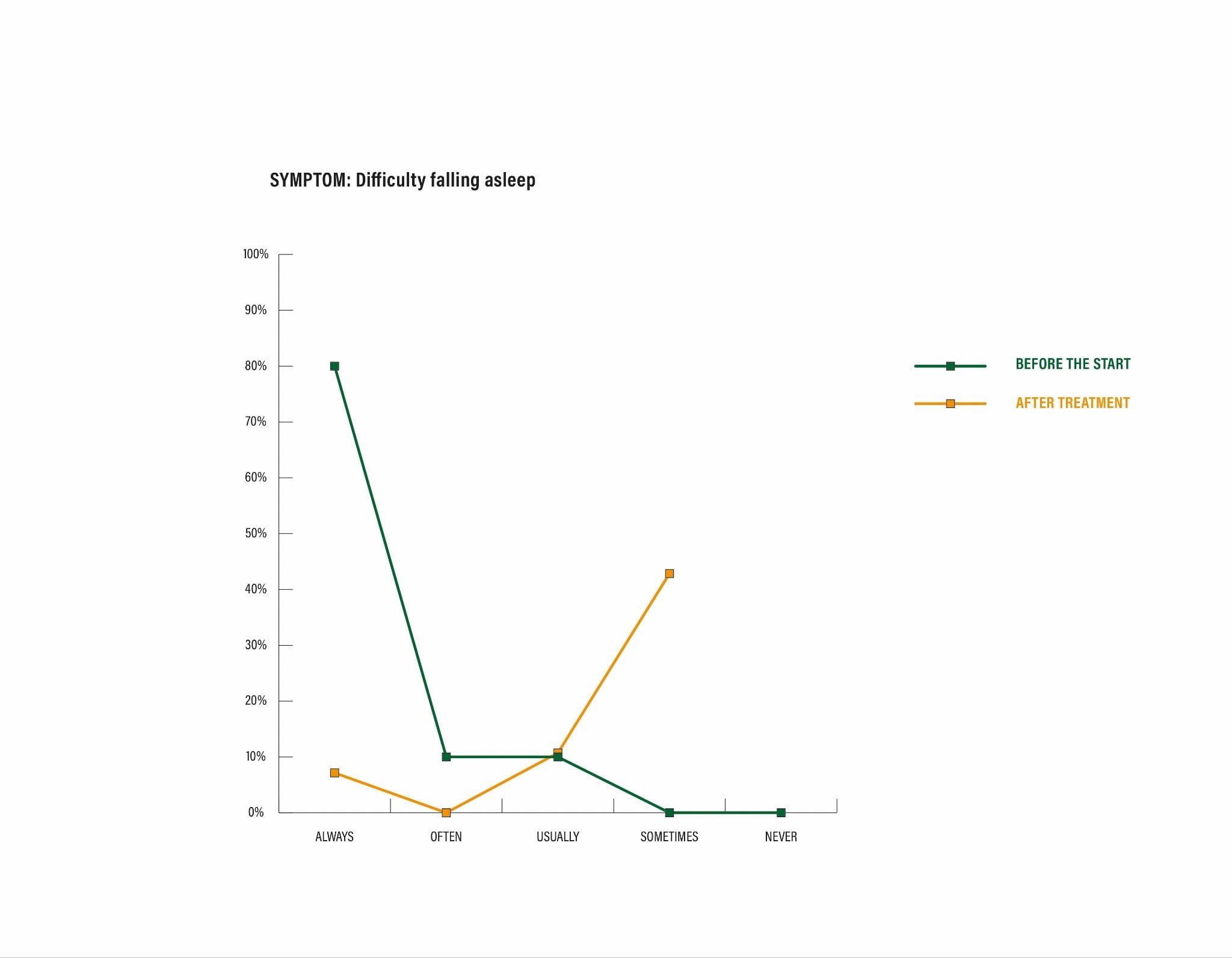
| 1 | Difficulty falling asleep at night | |||||
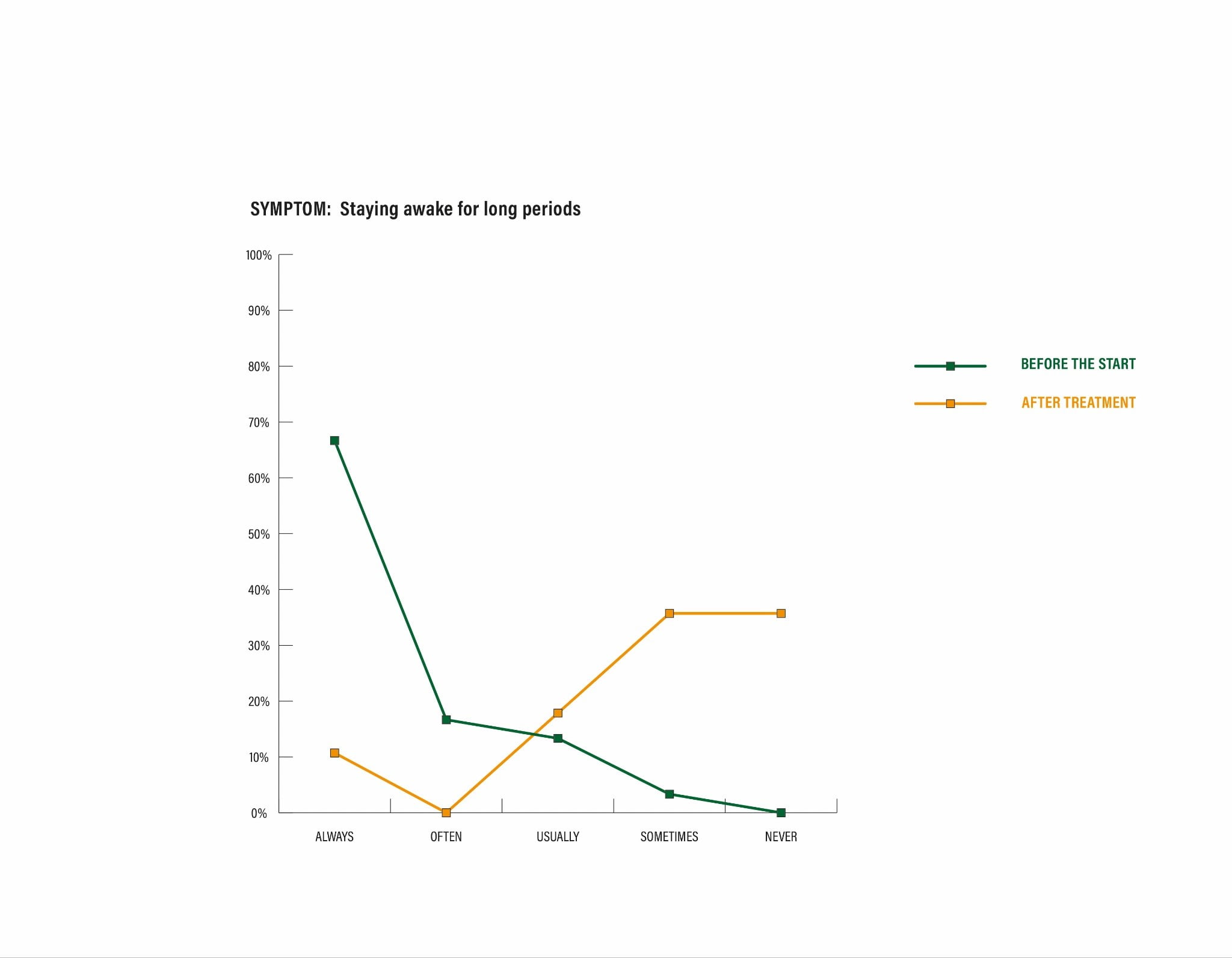
| 2 | Staying awake for long periods of time during the night (specify for how long) | |||||
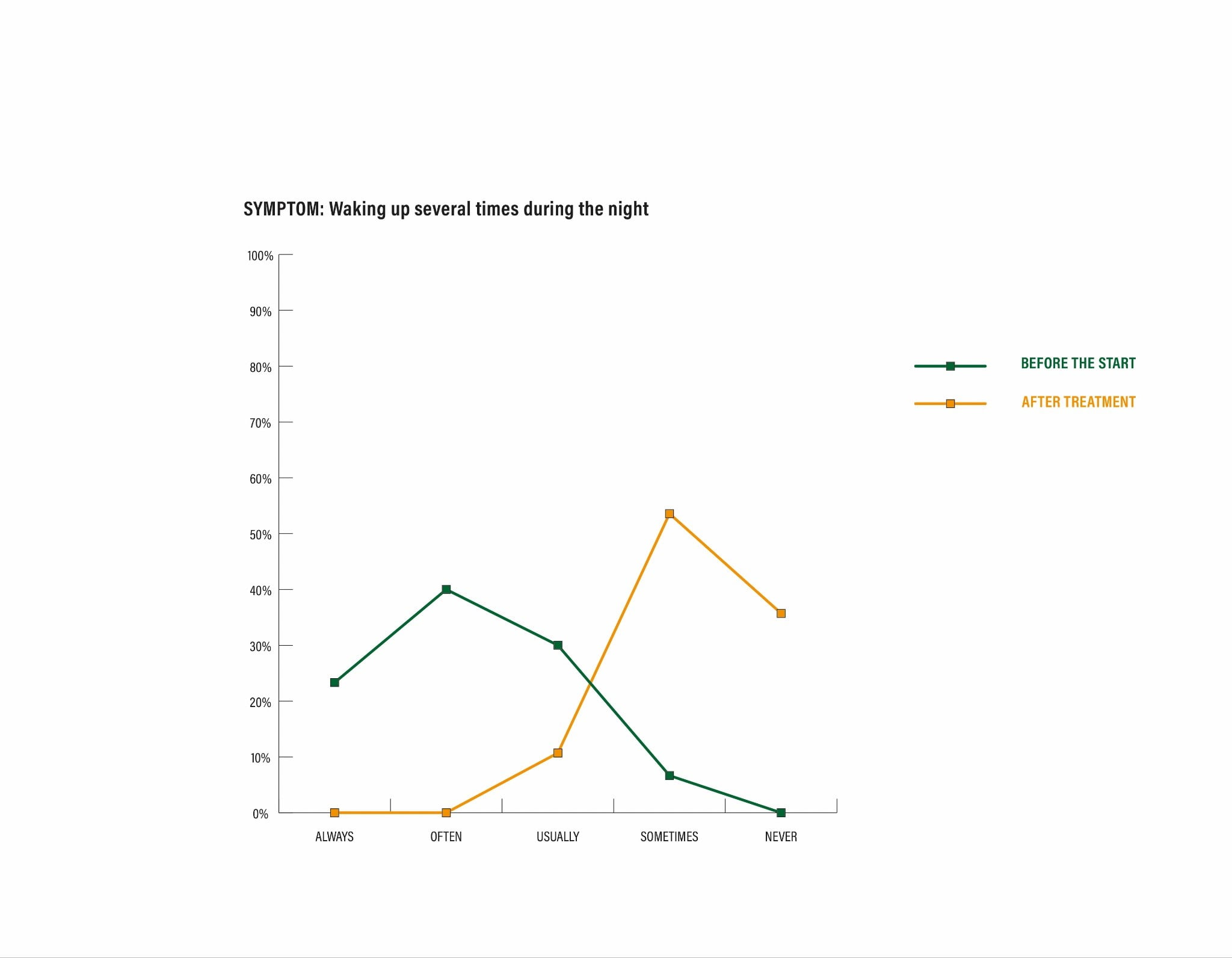
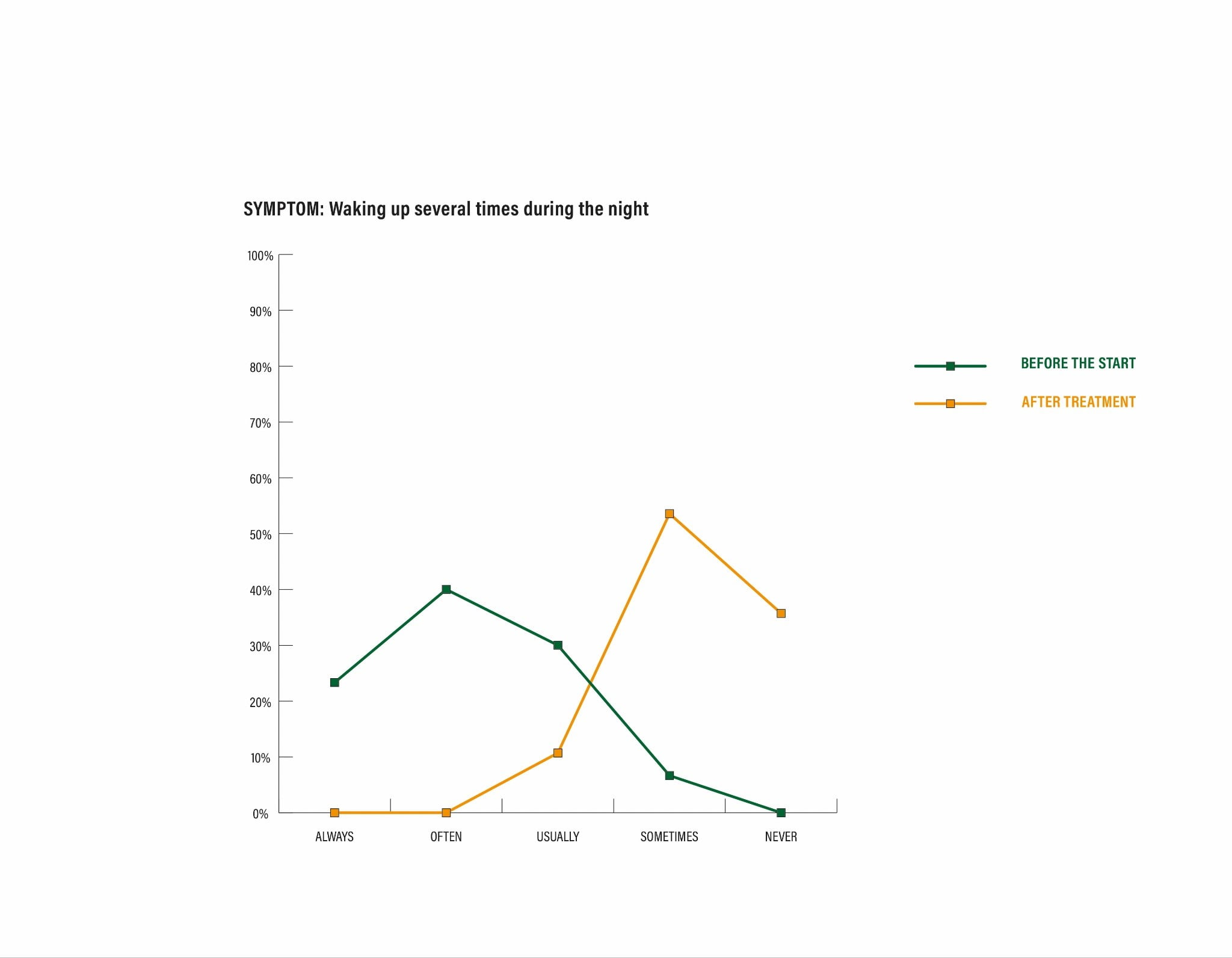
| 3 | Waking up several times during the night (specify how many times) | |||||
| 4 | Waking up early in the morning without being able going back to sleep again (specify at what time). | |||||
| 5 | Not feeling refreshed after sleep. Rate from 1 (not tired at all) to 10 (exhausted) Specify how tired you actually feel. |
|||||
| 6 | Feeling fatigued or sleepy during the day. Rate from 1 (no fatigue) to 10 (extreme fatigue) | |||||
| 7 | Having difficulty concentrating on a task. | |||||
| 8 | Feeling irritable, roughly from 1 (not irritable at all) to 10 (maximum irritability). | |||||
| 9 | Regular medical treatment. (Note modification, if any, during the study) |
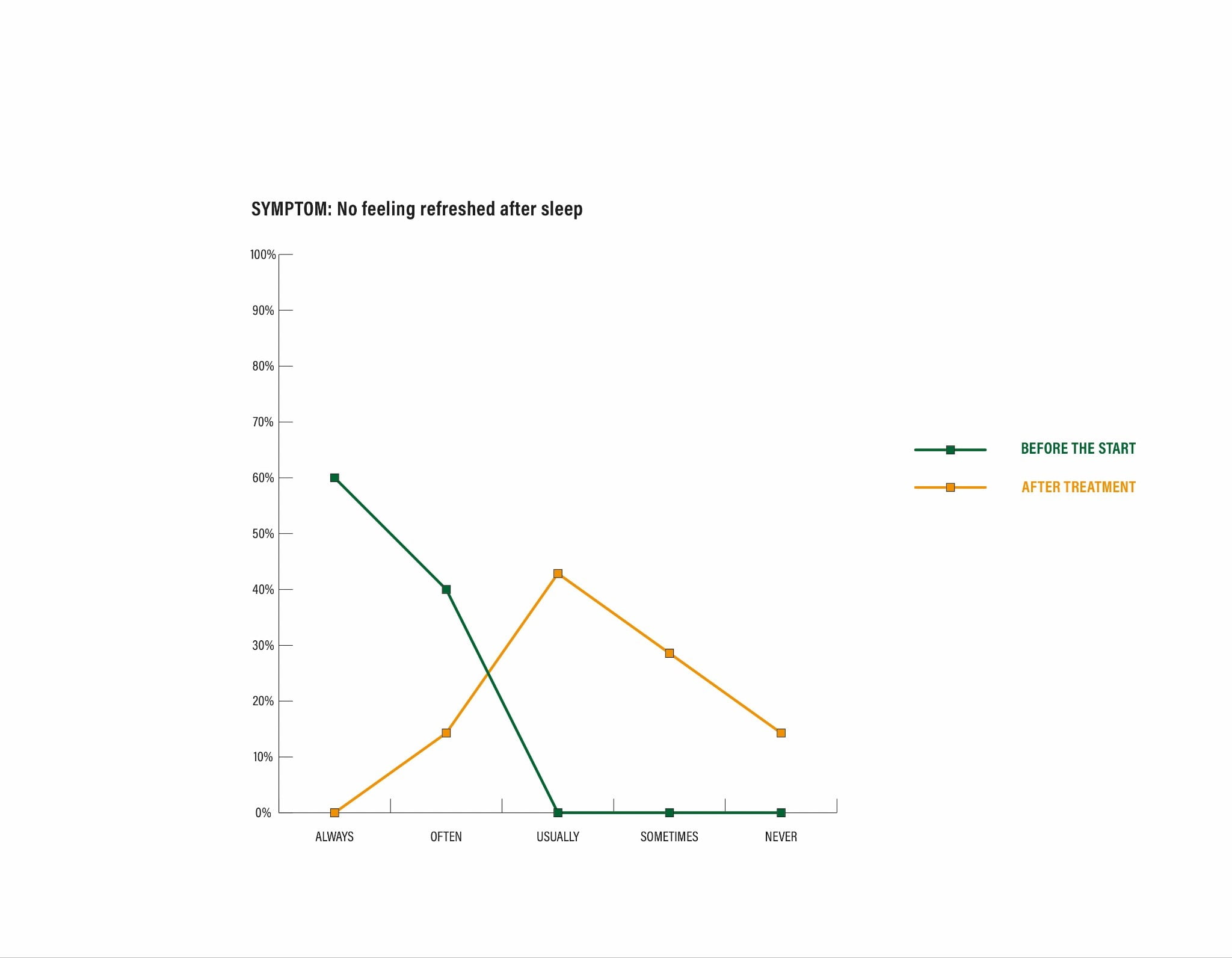
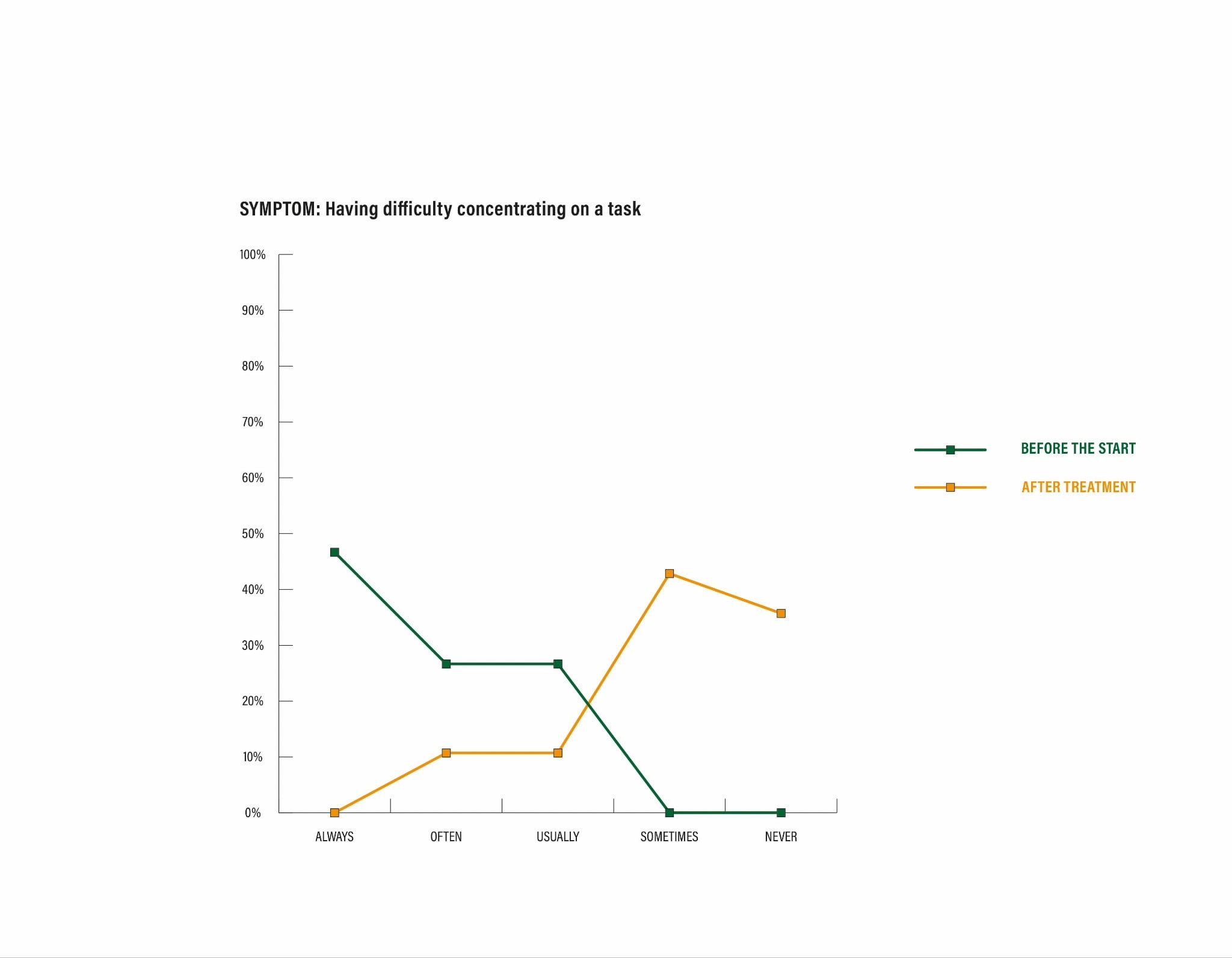
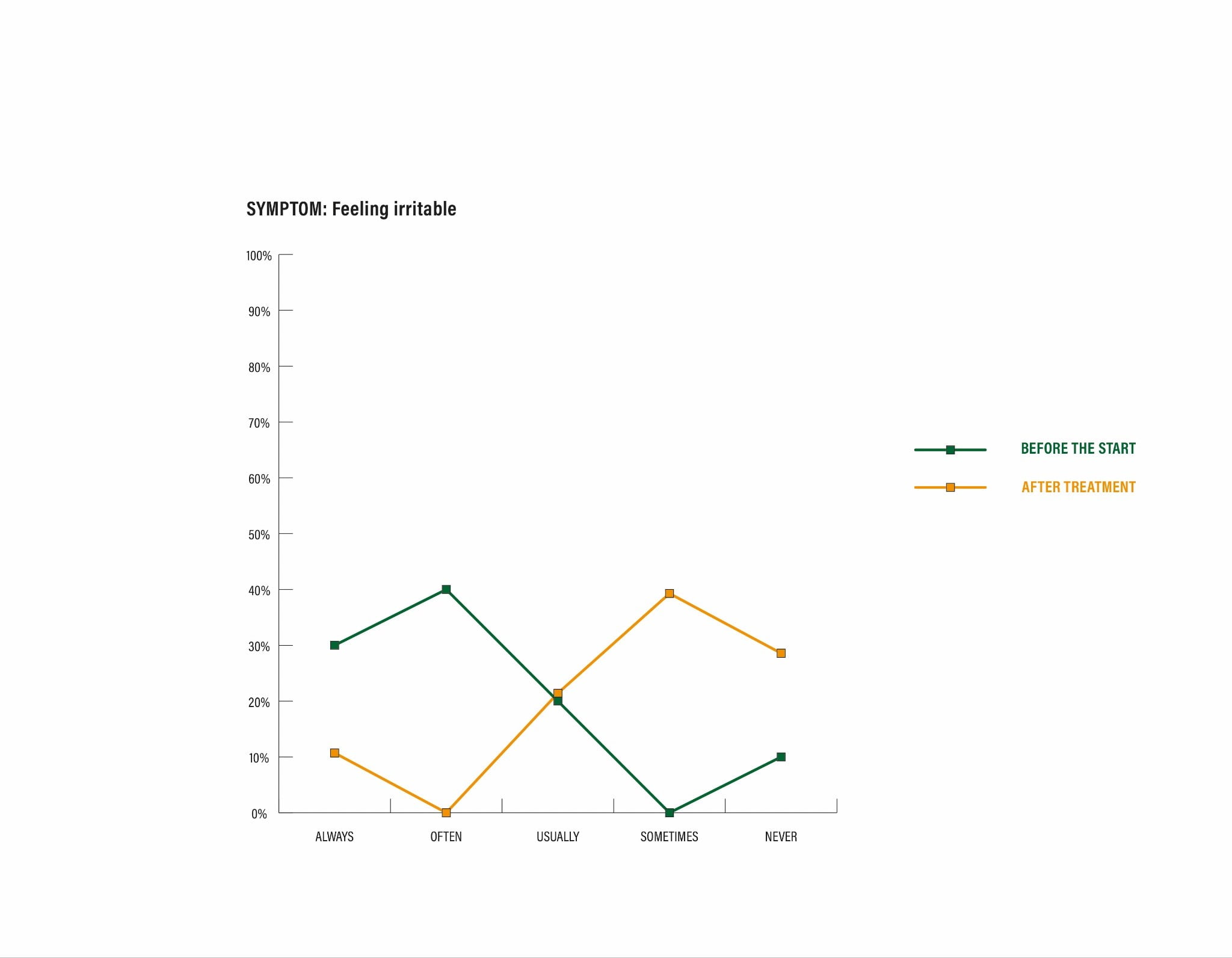
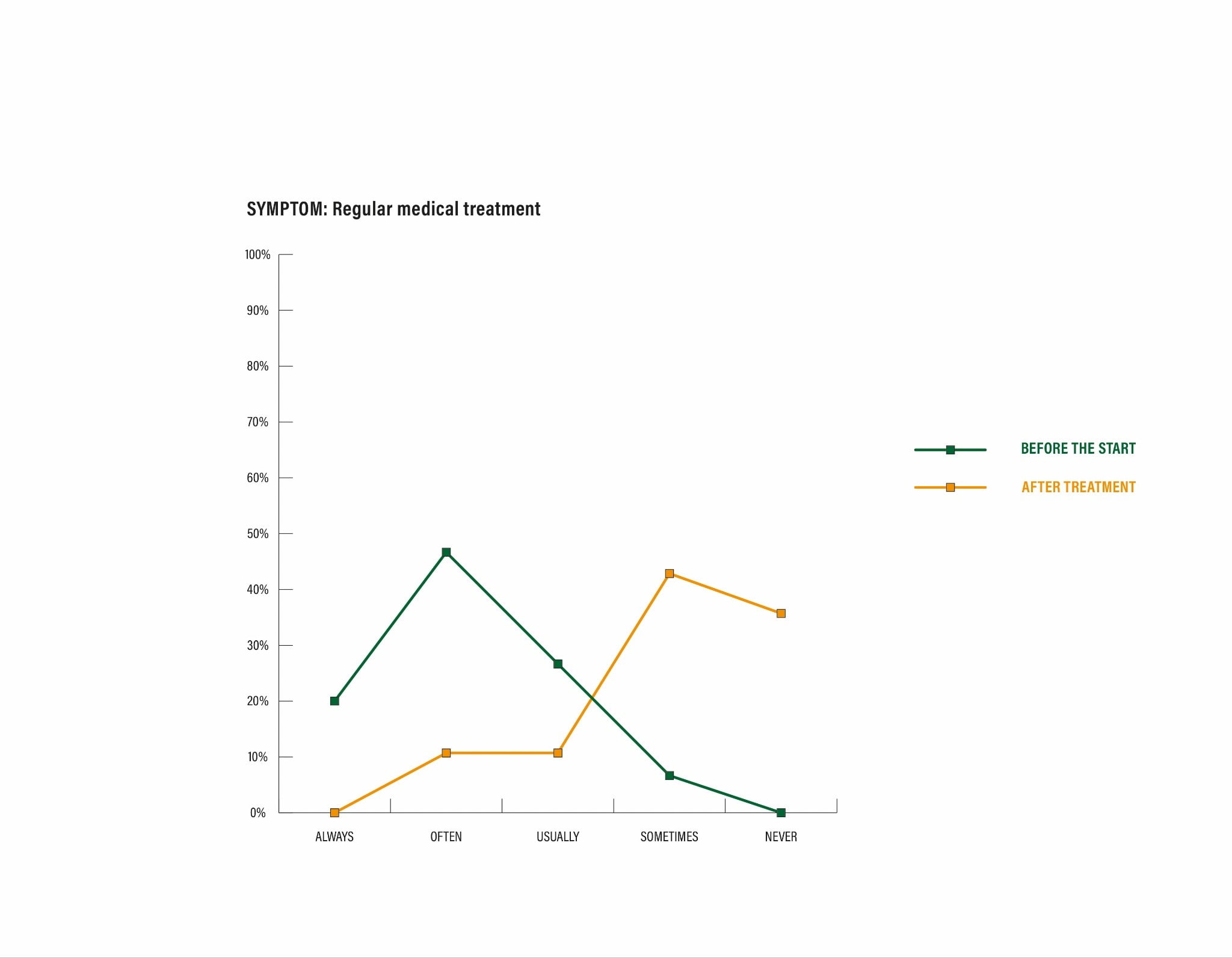
Chart of symptoms recorded at the beginning and end of the present work. Below are the graphs resulting from crossing the coordinates, for example: Symptom 1 “Difficulty falling asleep at night”, with the data collected from the patients’ responses in relation to the intensity and frequency of the presentation of this symptom. In grey, the data at the beginning of the study and in red, the data collected at the end of the study, in each case.
Results and findings
A change in the appearance of symptoms, both in frequency and intensity, has been observed and documented in the preceding graphs. There, it can be seen how the initial symptoms (grey bar) appear frankly lateralized to the left of the coordinates. This shows how, at the beginning of the study, the symptoms and discomfort related to this pathology were categorically frequent and intense.
On the other hand, it has been observed and documented how the symptoms at the end of the follow-up (red bar) appear in a greater proportion to the right, which corresponds to their disappearance or reduction. Thus, demonstrating a marked symptomatic reduction in the eight patients who completed the three sessions scheduled at the beginning of the study. In some of them, the improvement was categorical; in others, the initial symptoms were reduced to a lesser degree.
There was no progress or deepening of the recorded symptoms in any of the cases under study.
Two volunteers abandoned the protocol (one for family reasons that prevented him or her from attending the session, and another claimed that “it is not the kind of therapy for me”). The first of them mentioned a subjective improvement after the end of the first session, although it could not be documented for the reasons previously mentioned. None of these volunteers reported a symptomatic increase after the first session.
Conclusion:
In light of the observation of these initial results, we believe that past-life regression therapy can be considered a valid tool when advancing towards an integral approach to the healing process of insomnia.
This work has marked a line of research to be followed. In spite of being a small sample, it is valid to call the attention of other researchers in order to recruit more volunteers for the “n” of this work. We call on teaching and research entities for funding. We believe that it is necessary to allocate economic and human resources in order to enlarge the sample. Furthermore, we are aware that our conclusions serve as a stepping stone for larger studies in order to extrapolate the results to the general population.
In view of the above-mentioned arguments and such encouraging results, we hope that more researchers will wish to join this project or the new lines of research resulting from it in order to provide the necessary scientific support for the validation of past-life regression therapy.
References:
Sarrais, F., & de Castro Manglano, P. (2007). El insomnio. Anales del Sistema Sanitario de Navarra. Scientific Electronic Library Online: SciELO Analytics (2007). Volume.30, suppl.1, pages 121-134. ISSN 1137-6627. Retrieve from: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1137-66272007000200011&lng=es&tlng=es
Terapia grupal cognitivo-conductual para el insomnio: evaluación de resultados tras su introducción en un departamento de salud. Journal: Revista de Neurología, Neurología.com. Editors: Viguera Editores. Volume 70 | Number 07 | Article Nº 16.689 | Download PDF Nº 336 | Published on April 1, 2020, pages 246- 250.
De Entrambasaguas M, Aiko-Gesler M, Luciano E, Domínguez-Cabañero EM, Terrés B, Diego-Castaño S, González-Vivas C, García- Parreño B, Lorente-Rovira E, Herraiz B, Victorio R, Cases- Bergón P., (2020), Terapia grupal cognitivo-conductual para el insomnio: evaluación de resultados tras su introducción en un departamento de salud. Journal: Revista de Neurología, Neurología.com. Editors: Viguera Editores | Volume70 | Number 07. Pages 246-250. Retrieved from: https://neurologia.com/articulo/2019385
Insomnia Overview: Epidemiology, Pathophysiology, Diagnosis and Monitoring, and Nonpharmacologic Therapy. Journal: The American Journal of Managed Care (AJMC). Volume 26, Issue 4.
Dopheide J. A. (2020). Insomnia overview: epidemiology, pathophysiology, diagnosis and monitoring, and nonpharmacologic therapy. Journal: The American Journal of Managed Care. Volume 26. Issue 4, S76–S84. Retrieved from: https://doi.org/10.37765/ajmc.2020.42769
Martínez HO, Montalván MO, Betancourt IY., (2019), Trastorno de insomnio. Consideraciones actuales. Journal: Revista Médica Electrónica. (2019); 41 (Edition N°2): pages 483-495. Retrieved from: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=88143
The American Psychiatric Association (APA). (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).
Diagnose Criteria DSM-5 780.52 (G47.00)